Gastric cancer (Stomach cancer)
Pathogenesis & Risk Factors of Gastric Adenocarcinoma
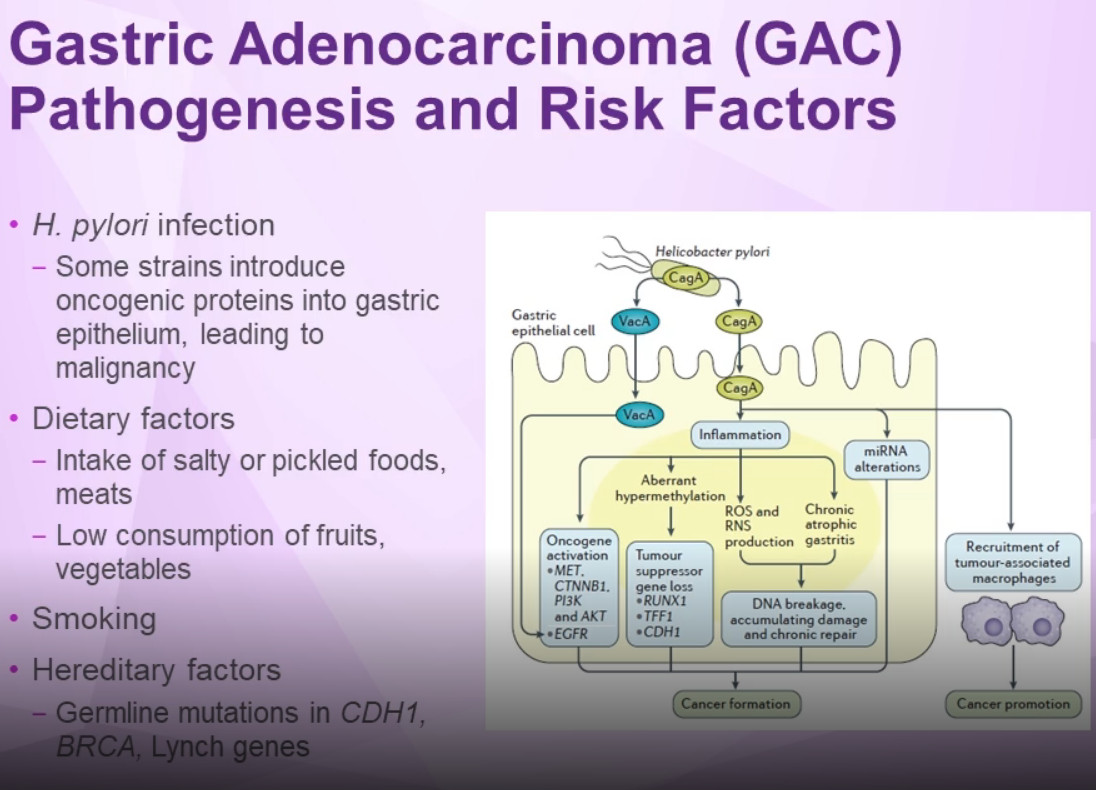
Some strains of H. pylori can introduce oncogenic proteins into the gastric epithelium; cytotoxin-associated gene A (CagA) can induce activation of oncogenes (MET, CTNNB1, PI3K, and AKT), aberrant hypermethylation resulting in loss of tumor suppressor genes (RUNX1, TFF1, and CDH1), and increased levels of reactive oxygen species (ROS), and reactive nitrogen species (RNS).1 Vacuolating cytotoxin A (VacA) activates eGFR, which also promotes cancer formation.
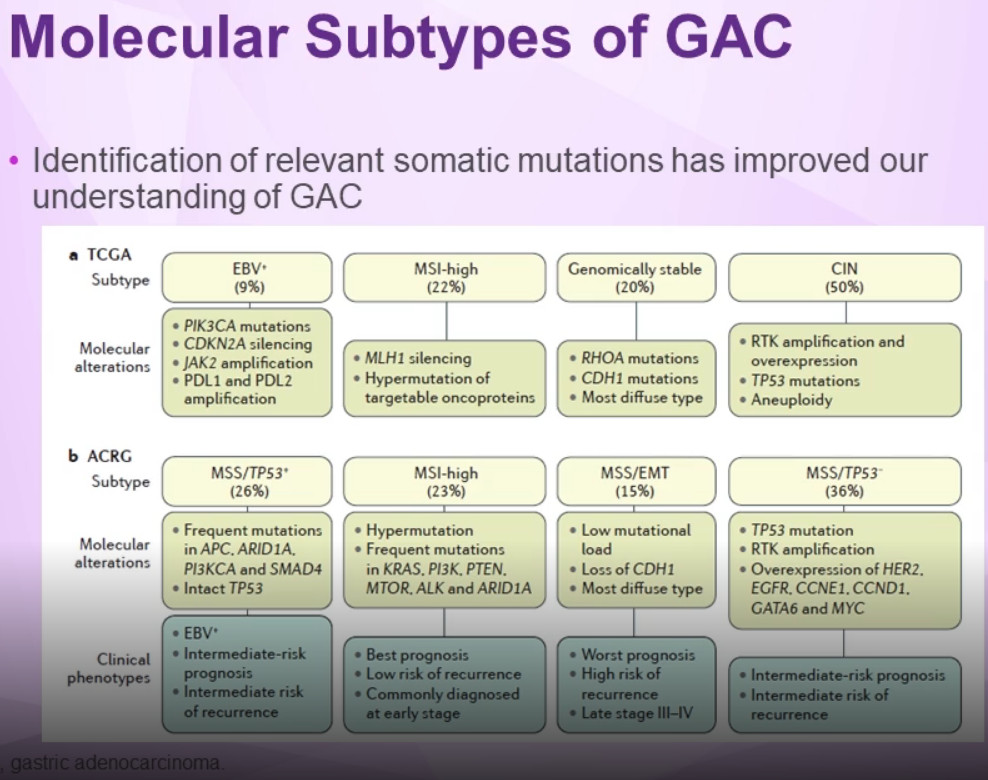
Molecular Subtypes of Gastric Cancer
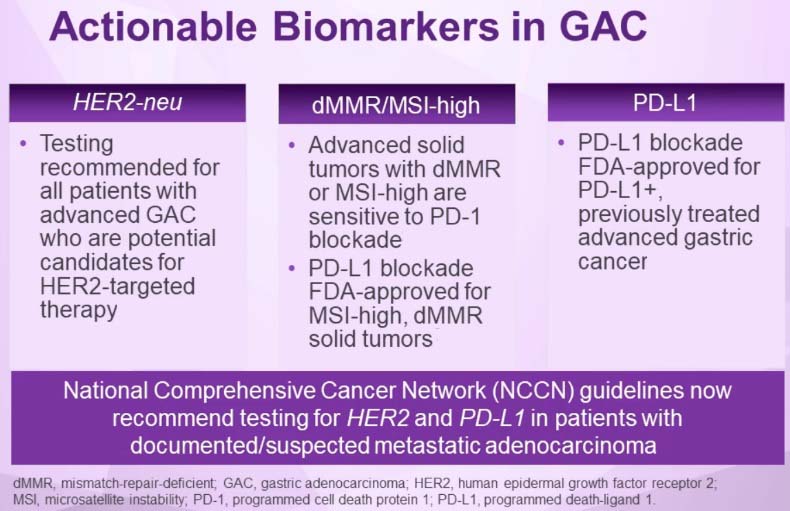
Actionable Biomarkers of Gastric Adenocarcinoma
NCCN Guildliness for Treatment of Gastric Adenocarcinoma
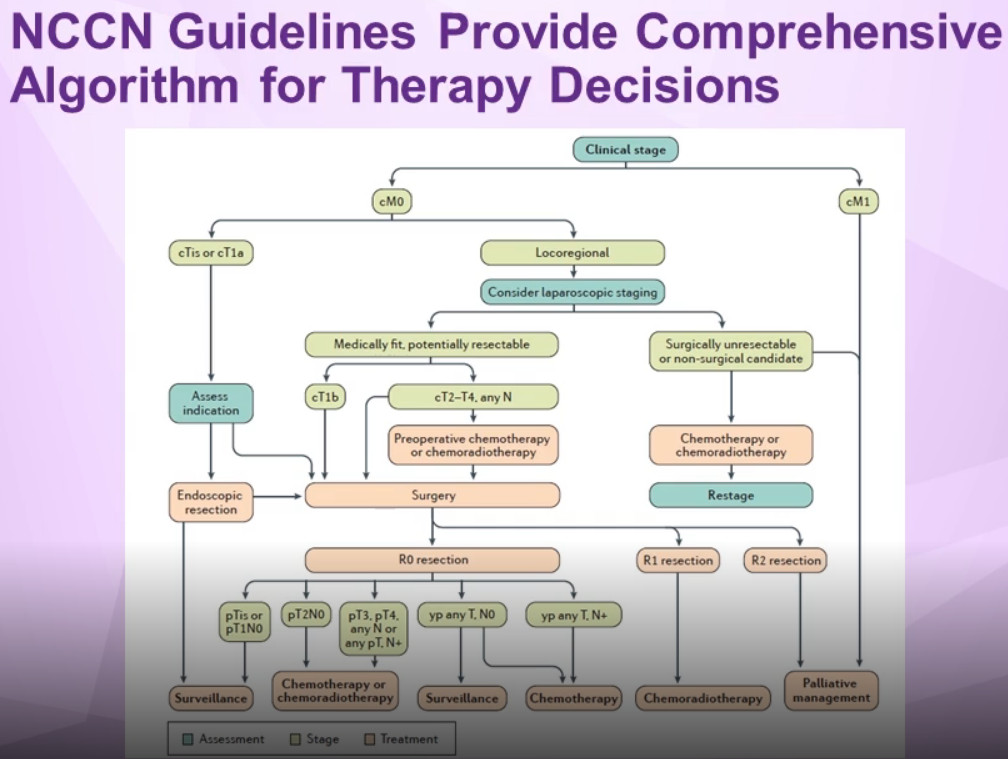
Treatment of gastric cancer
Stomach cancer may be treated with surgery, radiation therapy, chemotherapy, targeted therapy, or immunotherapy... Often, a combination of these treatments is used. It can be difficult to cure stomach cancer because it is often not found until it is at an advanced stage.
Treatment options and recommendations depend on several factors, including the type and stage of cancer, possible side effects, and the patient’s preferences and overall health. Your care plan may also include treatment for symptoms and side effects, an important part of cancer care.
Surgery
The type of surgery used depends on the stage of the cancer (see Stages).
For a very early stage (T1a) cancer, some doctors may recommend a non-surgical treatment called endoscopic mucosal resection. This is the removal of the tumor with an endoscope.
In early stages (stages 0 or I), when the cancer is still only in the stomach, surgery is used to remove the part of the stomach with cancer and nearby lymph nodes. This is called a subtotal or partial gastrectomy. In a partial gastrectomy, the surgeon connects the remaining part of the stomach to the esophagus or small intestine.
If the cancer has spread to the outer stomach wall with or without having spread to the lymph nodes, surgery plus chemotherapy or chemotherapy and radiation therapy may be used. The surgeon can perform a subtotal gastrectomy or a total gastrectomy. During a total gastrectomy, the surgeon attaches the esophagus directly to the small intestine.
Gastrectomy is a major surgery and can have serious side effects. After this surgery, the patient will only be able to eat a small amount of food at a time. A common side effect is a group of symptoms known as dumping syndrome, which includes cramps, nausea, diarrhea, and dizziness after eating. This happens when food enters the small intestine too fast. The doctor can suggest ways to avoid this and can prescribe medication to help control these symptoms. The symptoms usually lessen or disappear in a few months, but they may be permanent for some people. Patients who have had their entire stomach removed may need regular injections of vitamin B12 because they may no longer be able to absorb this essential vitamin through their stomach.
Regional lymph nodes are often removed during surgery because the cancer may have spread to those lymph nodes. This is called a lymphadenectomy. There is still debate as to how many lymph nodes should be removed. In Europe and especially in Japan, more lymph nodes are removed than in the United States.
When the cancer is diagnosed as Stage IV, surgery is typically not recommended as the main treatment (see Metastatic stomach cancer, below).
Radiation therapy
Patients with stomach cancer usually receive external-beam radiation therapy. Radiation therapy may be used before surgery to shrink the size of the tumor or after surgery to destroy any remaining cancer cells.
Chemotherapy
The goal of chemotherapy can be to destroy cancer remaining after surgery, slow the tumor’s growth, or reduce cancer-related symptoms. It also may be combined with radiation therapy. Currently, there is no single standard chemotherapy treatment regimen that is used worldwide. However, most chemotherapy treatments for stomach cancer are based on the combination of at least 2 drugs:
• Cisplatin (Platinol) • Fluorouracil (5-FU, Adrucil)
Other drugs used include:
• Capecitabine (Xeloda) • Docetaxel (Docefrez, Taxotere) • Epirubicin (Ellence) • Irinotecan (Camptosar) • Oxaliplatin (Eloxatin) • Paclitaxel (Taxol)
Targeted therapy
Targeted therapy is a treatment that targets the cancer’s specific genes, proteins, or the tissue environment that contributes to cancer growth and survival. This type of treatment blocks the growth and spread of cancer cells while limiting damage to healthy cells.
Recent studies show that not all tumors have the same targets. To find the most effective treatment, your doctor may run tests to identify the genes, proteins, and other factors in your tumor. This helps doctors better match each patient with the most effective treatment whenever possible. In addition, many research studies are taking place now to find out more about specific molecular targets and new treatments directed at them.
• HER2-targeted therapy. Some cancers may make too much of the protein called human epidermal growth factor receptor 2 (HER2). This type of cancer is called HER2-positive cancer. Trastuzumab (Herceptin) plus chemotherapy may be an option for patients with later-stage HER2-positive stomach cancer.
• Anti-angiogenesis therapy. Anti-angiogenesis therapy is a type of targeted therapy. It is focused on stopping angiogenesis, which is the process of making new blood vessels. Because a tumor needs the nutrients delivered by blood vessels to grow and spread, the goal of anti-angiogenesis therapies is to “starve” the tumor. For patients whose tumor has grown while receiving initial chemotherapy, the drug ramucirumab (Cyramza) may be an additional option.
Immunotherapy
Immunotherapy, also called biologic therapy, is designed to boost the body's natural defenses to fight the cancer. It uses materials made either by the body or in a laboratory to improve, target, or restore immune system function. This is an active area of research for stomach cancer.
Treatment Choices by Type and Stage of Stomach Cancer
Treatment of stomach cancer depends to a large degree on where the cancer started in the stomach and how far it has spread.
Stomach cancers can grow and spread in different ways. They can grow through the wall of the stomach and invade nearby organs. They can also spread to the lymph vessels and nearby lymph nodes (bean-sized structures that help fight infections). The stomach has a very rich network of lymph vessels and nodes. As the stomach cancer becomes more advanced, it can travel through the bloodstream and spread (metastasize) to organs such as the liver, lungs, and bones, which can make it harder to treat.
Stage 0
Because stage 0 cancers are limited to the inner lining layer of the stomach and have not grown into deeper layers, they can be treated by surgery alone.
Surgery with either subtotal gastrectomy (removal of part of the stomach) or total gastrectomy is often the main treatment for these cancers. Nearby lymph nodes are removed as well.
Some small stage 0 cancers can be treated by endoscopic resection. This is done more often in Japan, where stomach cancer is often detected early during screening. It is rare to find stomach cancer so early in the United States, so this treatment has not been used as much here. If it is done, it should be at a cancer center that has a great deal of experience with this technique.
Stage I
Stage IA: People with stage IA stomach cancer typically have their cancer removed by total or subtotal gastrectomy. The nearby lymph nodes are also removed. Endoscopic resection may rarely be an option for some small T1a cancers. No further treatment is usually needed after surgery.
Stage IB: The main treatment for this stage of stomach cancer is surgery (total or subtotal gastrectomy). Chemotherapy (chemo) or chemoradiation (chemo plus radiation therapy) may be given before surgery to try to shrink the cancer and make it easier to remove.
After surgery, patients whose lymph nodes (removed at surgery) show no signs of cancer spread are sometimes observed without further treatment, but often doctors will recommend treatment with either chemoradiation or chemo alone after surgery (especially if the patient didn’t get one of these before surgery). Patients who were treated with chemo before surgery may get the same chemo (without radiation) after surgery.
If cancer is found in the lymph nodes, treatment with either chemoradiation, chemo alone, or a combination of the two is often recommended.
If a person is too sick (from other illnesses) to have surgery, they may be treated with chemoradiation if they can tolerate it. Other options include radiation therapy or chemo alone.
Stage II
The main treatment for stage II stomach cancer is surgery to remove all or part of the stomach, the omentum, and nearby lymph nodes. Many patients are treated with chemo or chemoradiation before surgery to try to shrink the cancer and make it easier to remove. Treatment after surgery may include chemo alone or chemoradiation.
If a person is too sick (from other illnesses) to have surgery, they may be treated with chemoradiation if they can tolerate it. Other options include radiation therapy or chemo alone.
Stage III
Surgery is the main treatment for patients with this stage disease (unless they have other medical conditions that make them too ill for it). Some patients may be cured by surgery (along with other treatments), while for others the surgery may be able to help control the cancer or help relieve symptoms.
Some people may get chemo or chemoradiation before surgery to try to shrink the cancer and make it easier to remove. Patients who get chemo before surgery will probably get chemo after, as well. For patients who don’t get chemo before surgery and for those who have surgery but have some cancer left behind, treatment after surgery is usually chemoradiation.
If a person is too sick (from other illnesses) to have surgery, they may be treated with chemoradiation if they can tolerate it. Other options include radiation therapy or chemo alone.
Stage IV
Because stage IV stomach cancer has spread to distant organs, a cure is usually not possible. But treatment can often help keep the cancer under control and help relieve symptoms. This might include surgery, such as a gastric bypass or even a subtotal gastrectomy in some cases, to keep the stomach and/or intestines from becoming blocked (obstructed) or to control bleeding.
In some cases, a laser beam directed through an endoscope (a long, flexible tube passed down the throat) can destroy most of the tumor and relieve obstruction without surgery. If needed, a stent (a hollow metal tube) may be placed where the esophagus and stomach meet to help keep it open and allow food to pass through it. This can also be done at the junction of the stomach and the small intestine.
Chemo and/or radiation therapy can often help shrink the cancer and relieve some symptoms as well as help patients live longer, but is usually not expected to cure the cancer. Combinations of chemo drugs are most commonly used, but which combination is best is not clear.
Targeted therapy can also be helpful in treating advanced stomach cancers. Trastuzumab (Herceptin) can be added to chemotherapy for patients whose tumors are HER2-positive. Ramucirumab (Cyramza) may also be an option at some point. It can be given by itself or added to chemo. The immunotherapy drug pembrolizumab (Keytruda) might also be an option at some point.
Because these cancers can be hard to treat, new treatments being tested in clinical trials may benefit some patients.
Recurrent cancer
Treatment options for recurrent disease are generally the same as they are for stage IV cancers. But they also depend on where the cancer recurs, what treatments a person has already had, and the person’s general health.
Clinical trials or newer treatments may be an option and should always be considered.
Treatment for Gastric Cancer
Treatment Option Overview for Gastric Cancer
Radical surgery represents the standard form of therapy that has curative intent. However, the incidences of local failure in the tumor bed and regional lymph nodes, and distant failures via hematogenous or peritoneal routes, remain high. As such, adjuvant external-beam radiation therapy with combined chemotherapy has been evaluated in the United States.
In a phase III Intergroup trial (SWOG-9008), 556 patients with completely resected stage IB to stage IV (M0) adenocarcinoma of the stomach and gastroesophageal junction were randomly assigned to receive surgery alone or surgery plus postoperative chemotherapy (5-fluorouracil [5-FU] and leucovorin) and concurrent radiation therapy (45 Gy).
With 5 years' median follow-up, a significant survival benefit was reported for patients who received adjuvant combined modality therapy. [Level of evidence: 1iiA]
Median survival was 36 months for the adjuvant chemoradiation therapy group and 27 months for the surgery-alone arm (P = .005).
Three-year overall survival (OS) rates were 50%, and relapse-free survival rates were 48% with adjuvant chemoradiation therapy versus 3-year OS rates of 41% and relapse-free survival rates of 31% for surgery alone (P = .005).
The rate of distant metastases was 18% for the surgery-alone arm and 33% for the chemoradiation-therapy arm.
Because distant disease remains a significant concern, the aim of the Cancer and Leukemia Group B study (CALGB-80101) was to augment the postoperative chemoradiation therapy regimen used in INT-0116. Neoadjuvant chemoradiation therapy such as in the RTOG-9904 trial, which is completed, and the SWOG-S0425 (NCT00335959) trial, which is closed, was clinically evaluated.
Investigators in Europe evaluated the role of preoperative and postoperative chemotherapy without radiation therapy.
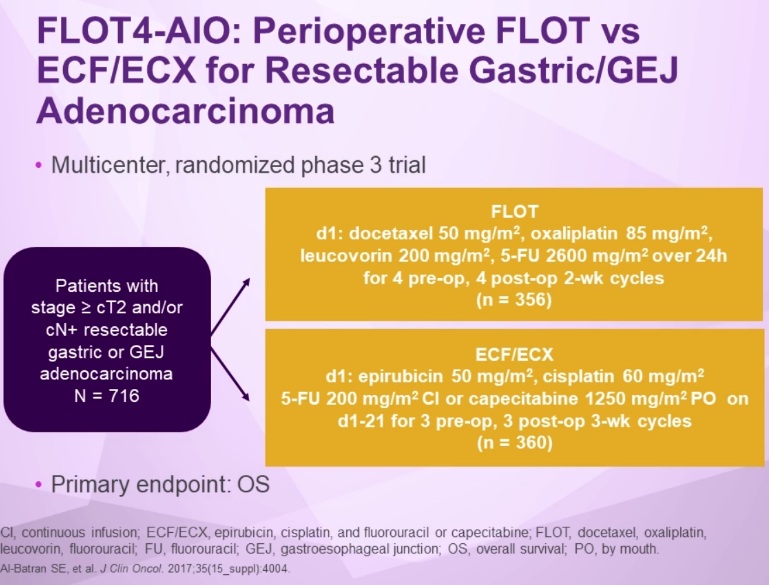
In the randomized phase III trial (MRC-ST02), patients with stage II or higher adenocarcinoma of the stomach or of the lower third of the esophagus were assigned to receive three cycles of epirubicin, cisplatin, and continuous infusion 5-FU before and after surgery or to receive surgery alone.
Compared with the surgery group, the perioperative chemotherapy group had a significantly higher likelihood of progression-free survival (hazard ratio [HR] for progression, 0.66; 95% confidence interval [CI], 0.53–0.81; P < .001) and of OS (HRdeath, 0.75; 95% CI, 0.60–0.93; P = .009).
Five-year OS was 36.3%; 95% CI, 29 to 43 for the perioperative chemotherapy group and 23%; 95% CI, 16.6 to 29.4 for the surgery group. [Level of evidence: 1iiA]
Standard Treatment Options for Gastric Cancer
Stage 0 Gastric Cancer
• Surgery.
Stage 0 is gastric cancer confined to mucosa. Experience in Japan, where stage 0 is diagnosed frequently, indicates that more than 90% of patients treated by gastrectomy with lymphadenectomy will survive beyond 5 years. An American series has confirmed these results.
Stage I Gastric Cancer
1. One of the following surgical procedures:
◦ Distal subtotal gastrectomy (if the lesion is not in the fundus or at the cardioesophageal junction).
◦ Proximal subtotal gastrectomy or total gastrectomy, both with distal esophagectomy (if the lesion involves the cardia). These tumors often involve the submucosal lymphatics of the esophagus.
◦ Total gastrectomy (if the tumor involves the stomach diffusely or arises in the body of the stomach and extends to within 6 cm of the cardia or distal antrum).
Regional lymphadenectomy is recommended with all of the above procedures. Splenectomy is not routinely performed.
(The role of extended lymph node (D2) dissection is uncertain and in some series is associated with increased morbidity.)
2. Postoperative chemoradiation therapy for patients with node-positive (T1 N1) and muscle-invasive (T2 N0) disease.
Stage II Gastric Cancer
1. One of the following surgical procedures:
◦ Distal subtotal gastrectomy (if the lesion is not in the fundus or at the cardioesophageal junction).
◦ Proximal subtotal gastrectomy or total gastrectomy (if the lesion involves the cardia).
◦ Total gastrectomy (if the tumor involves the stomach diffusely or arises in the body of the stomach and extends to within 6 cm of the cardia).
Regional lymphadenectomy is recommended with all of the above procedures. Splenectomy is not routinely performed.
2. Postoperative chemoradiation therapy.
A prospective multi-institution phase III trial (SWOG-9008) evaluated postoperative combined chemoradiation therapy versus surgery alone in 556 patients with completely resected stage IB to stage IV (M0) adenocarcinoma of the stomach and gastroesophageal junction and reported a significant survival benefit with adjuvant combined modality therapy.[Level of evidence: 1iiA] (See above)
(Note: Neoadjuvant chemoradiation therapy remains under clinical evaluation, such as in the SWOG-S0425 (NCT00335959) trial, which is closed and the RTOG-9904 trial, which is completed.)
3. Perioperative chemotherapy.
In the randomized phase III trial (MRC-ST02), patients with stage II or higher adenocarcinoma of the stomach or of the lower third of the esophagus were assigned to receive three cycles of epirubicin, cisplatin, and continuous infusion fluorouracil (ECF) before and after surgery or to receive surgery alone.
◦ Compared with the surgery group, the perioperative chemotherapy group had a significantly higher likelihood of progression-free survival (hazard ratio [HR] for progression, 0.66; 95% confidence interval [CI], 0.53–0.81; P < .001) and of OS (HR for death, 0.75; 95% CI, 0.60–0.93; P = .009).
◦ Five-year OS was 36.3%, 95% CI, 29 to 43 for the perioperative chemotherapy group and 23%, 95% CI, 16.6 to 29.4 for the surgery group. [Level of evidence: 1iiA]
4. Postoperative chemotherapy.
. Japanese investigators randomly assigned 1,059 patients with stage II or III gastric cancer who had undergone a D2 gastrectomy to receive either 1 year of fluoropyrimidine or follow-up after surgery alone.
Patients were randomly assigned in a 1:1 fashion.
◦ The 3-year OS rate was 80.1% in the S-1 group and 70.1% in the surgery-only group. The HR for death in the S-1 group, as compared with the surgery-only group, was 0.68 (95% CI, 0.52–0.87; P = .003). [Level of evidence: 1iiA]
Subsequently, investigators in Asia evaluated the role of capecitabine/oxaliplatin as adjuvant therapy after gastric cancer resection.
In the CLASSIC (NCT00411229) trial, 37 centers in South Korea, China, and Taiwan randomly assigned 1,035 patients with stage IIA, IIB, IIIA, or IIIB gastric cancer who had undergone a curative D2 gastrectomy to receive adjuvant chemotherapy (eight 3-week cycles of capecitabine plus oxaliplatin) or follow-up post-surgery alone.
◦ The 3-year disease-free survival rate was 74% in the chemotherapy group and 59% in the surgery-alone group (HR, 0.56; 95% CI, 0.44–0.72; P < .0001).
◦ The 3-year OS was 83% in the chemotherapy group and 78% in the surgery-alone group (HR, 0.72; 95% CI, 0.52–1.00; P = .0493). [Level of evidence: 1iiA]
◦ Further follow-up is anticipated.
Stage III Gastric Cancer
1. Radical surgery. Curative resection procedures are confined to patients who do not have extensive nodal involvement at the time of surgical exploration.
Surgery is the treatment of choice for all patients who have tumors that can be resected. As many as 15% of selected stage III patients can be cured by surgery alone, particularly if lymph node involvement is minimal (<7 lymph nodes).
2. Postoperative chemoradiation therapy.
Same as Stage II.
3. Perioperative chemotherapy.
Same as Stage II.
4. Postoperative chemotherapy.
Same as Stage II.
Stage IV and Recurrent Gastric Cancer
1. Palliative chemotherapy with:
◦ Fluorouracil (5-FU) ◦ Epirubicin, cisplatin, and 5-FU (ECF) ◦ Epirubicin, oxaliplatin, and capecitabine (EOX) ◦ Cisplatin and 5-FU (CF) ◦ Docetaxel, cisplatin, and 5-FU ◦ Etoposide, leucovorin, and 5-FU (ELF) ◦ 5-FU, doxorubicin, and methotrexate (FAMTX).
2. Trastuzumab, cisplatin, and either 5-FU or capecitabine in patients with HER2-positive tumors (3+ on immunohistochemistry [IHC] or fluorescence in situ hybridization [FISH]-positive).
3. Endoluminal laser therapy, endoluminal stent placement, or gastrojejunostomy, may be helpful to patients with gastric obstruction.
4. Palliative radiation therapy may alleviate bleeding, pain, and obstruction.
5. Palliative resection is reserved for patients with continued bleeding or obstruction.
Standard chemotherapy versus best supportive care for patients with metastatic gastric cancer has been tested in several clinical trials, and there is general agreement that patients who receive chemotherapy live for several months longer on average than patients who receive supportive care. [Level of evidence: 1iiA]
During the last 20 years, multiple randomized studies evaluating different treatment regimens (monotherapy vs. combination chemotherapy) have been performed in patients with metastatic gastric cancer with no clear consensus emerging as to the best management approach. A meta-analysis of these studies demonstrated a hazard ratio (HR) of 0.83 for overall survival (OS) (95% confidence interval [CI], 0.74–0.93) in favor of combination chemotherapy.
1. Of all the combination regimens, ECF is often considered the reference standard in the United States and Europe. In one European trial, 274 patients with metastatic esophagogastric cancer were randomly assigned to receive either ECF or FAMTX.
◦ The group who received ECF had a significantly longer median survival (8.9 vs. 5.7 months, P = .0009) than the FAMTX group. [Level of evidence: 1iiA]
2. In a second trial that compared ECF with mitomycin, cisplatin, and 5-FU (MCF), there was no statistically significant difference in median survival (9.4 vs. 8.7 months, P = .315). [Level of evidence: 1iiA]
3. Oxaliplatin and capecitabine are often substituted for cisplatin and 5-FU within the ECF regimen on the basis of results from the REAL-2 trial (ISRCTN51678883). This randomized trial of 1,002 patients with advanced esophageal, gastroesophageal (GE) junction, or gastric cancer utilized a 2 × 2 design to demonstrate noninferior median OS in patients treated with capecitabine rather than 5-FU (HRdeath = 0.86; 95% CI, 0.82–0.99) and in patients treated with oxaliplatin in place of cisplatin (HRdeath = 0.92; 95% CI, 0.80–1.10).
4. An international collaboration of investigators randomly assigned 445 patients with metastatic gastric cancer to receive docetaxel, cisplatin, and 5-FU (DCF) or CF. Time-to-treatment progression (TTP) was the primary endpoint.
◦ Patients who received DCF experienced a significantly longer TTP (5.6 months; 95% CI, 4.9–5.9; vs. 3.7 months; 95% CI, 3.4–4.5; HR, 1.47; 95% CI, 1.19–1.82; log-rank P < .001; risk reduction 32%).
◦ The median OS was significantly longer for patients who received DCF versus patients who received CF (9.2 months; 95% CI, 8.4–10.6; vs. 8.6 months; 95% CI, 7.2–9.5; HR, 1.29; 95% CI, 1.0–1.6; log-rank P = .02; risk reduction = 23%). [Level of evidence: 1iiA]
◦ There were high toxicity rates in both arms.
◦ Febrile neutropenia was more common in patients who received DCF (29% vs. 12%), and the death rate on the study was 10.4% for patients on the DCF arm and 9.4% for patients on the CF arm.
5. Whether the CF regimen should be considered as an index regimen for the treatment of patients with metastatic gastric cancer is the subject of debate. The results of a study that randomly assigned 245 patients with metastatic gastric cancer to receive CF, FAMTX, or ELF demonstrated no significant difference in response rate, progression-free survival, or OS between the arms.
◦ Grades 3 and 4 neutropenia occurred in 35% to 43% of patients on all arms, but severe nausea and vomiting was more common in patients in the CF arm and occurred in 26% of those patients.[7][Level of evidence: 1iiDiv]
Trastuzumab
In the open-label, international phase III ToGA (Trastuzumab for Gastric Cancer [NCT01041404]) trial, patients with HER2-positive metastatic, inoperable locally advanced, or recurrent gastric or GE junction cancer were randomly assigned to chemotherapy with or without the anti-HER2 monoclonal antibody trastuzumab.
HER2 positivity was defined as either 3+ staining by IHC or a HER2 to CEP17 ratio of two or more using FISH. Tumors from 3,665 patients were HER2 tested; of the patients, 810 were positive (22%) and 594 met eligibility criteria for randomization. Chemotherapy consisted of cisplatin plus 5-FU or capecitabine chosen at the investigator’s discretion. The study treatment was administered every 3 weeks for six cycles, and trastuzumab was continued every 3 weeks until disease progression, unacceptable toxicity, or withdrawal of consent. Crossover to trastuzumab at disease progression was not permitted.
◦ Median OS was 13.8 months (95% CI, 12–16) in patients assigned to trastuzumab and 11.1 months (95% CI, 10–13) in patients assigned to chemotherapy alone (HR, 0.74; 95% CI, 0.60–0.91; P = .0046). [Level of evidence: 1iiA]
◦ There was no significant difference in rates of any adverse event, and cardiotoxic effects were equally rare in both arms.
Second-line Chemotherapy
When patients develop progression of disease after first-line chemotherapy, there is no standard treatment option.
1. Investigators in Korea randomly assigned patients with advanced gastric cancer who had received one or two prior chemotherapy regimens involving both a fluoropyrimidine and a platinum agent to either salvage chemotherapy or best supportive care in a 2:1 fashion. Salvage chemotherapy consisted of either docetaxel (60 mg/m2 every 3 weeks) or irinotecan (150 mg/m2 every 2 weeks) and was left to the discretion of the treating physicians. Of the 202 patients enrolled, 133 received salvage chemotherapy and 69 received best supportive care.
◦ Median OS was 5.3 months in the group that received salvage chemotherapy and 3.8 months in the group that received best supportive care (HR, 0.657; P = .007).
◦ There was no difference in median OS between docetaxel and irinotecan (5.2 months vs. 6.5 months, P = .116).[Level of evidence: 1iiA]
Ramucirumab
Ramucirumab is a fully humanized monoclonal antibody directed against the vascular endothelial growth factor receptor-2.
1. In the international, phase III, placebo-controlled, REGARD trial (NCT00917384), 355 patients with stage IV gastric or GE junction cancer who had progressed on a first-line fluorouracil- or platinum-containing regimen were randomly assigned in a 2:1 fashion to ramucirumab or placebo.
◦ Patients who were assigned to ramucirumab had a significantly improved median OS of 5.2 months compared with patients assigned to the placebo who had a median OS of 3.8 months (HR, 0.776; P = .047).
◦ Rates of hypertension were higher in the ramucirumab group than in the placebo group. [Level of evidence: 1iiA]
Ramucirumab is an acceptable treatment in cisplatin or 5-FU refractory, stage IV, gastric cancer.
2. In the international, double-blinded, phase III RAINBOW trial (NCT01170663), 665 patients were randomly assigned to receive paclitaxel (80 mg/m2) on days 1, 8, and 15 every 28 days with ramucirumab (8 mg/kg) added on days 1 and 15 or a placebo added on days 1 and 15.
◦ Patients assigned to ramucirumab had a significant improvement in median OS of 9.6 months compared with patients assigned to a placebo who had a median OS of 7.4 months (HR, 0.807; P = .017).
◦ Grade 3 or higher neutropenia, fatigue, hypertension, and abdominal pain were more common in the ramucirumab group. [Level of Evidence: 1iA]
The combination of paclitaxel and ramucirumab is an acceptable second-line-chemotherapy regimen in patients with stage IV gastric or GE junction cancer.
Treatment options under clinical evaluation:
• Palliative chemotherapy with:
◦ Irinotecan and cisplatin ◦ Folic acid, 5-FU, and irinotecan (FOLFIRI) ◦ Leucovorin, 5-FU, and oxaliplatin (FOLFOX).
Phase II studies evaluating irinotecan-based or oxaliplatin-based regimens demonstrate similar response rates and TTP to those found with ECF or CF, but the former may be less toxic. There are conflicting data regarding relative efficacy of any one regimen. Ongoing studies are evaluating these newer regimens.