Colon Cancer
Cancer of the colon is a highly treatable and often curable disease when localized to the bowel. Surgery is the primary form of treatment and results in cure in approximately 50% of the patients. Recurrence following surgery is a major problem and is often the ultimate cause of death.
Incidence and Mortality
Estimated new cases and deaths from colon cancer in the United States in 2018:
• New cases: 97,220 (colon cancer only). • Deaths: 50,630 (colon and rectal cancers combined).
Gastrointestinal stromal tumors can occur in the colon. (Refer to the PDQ summary on Gastrointestinal Stromal Tumors Treatment for more information.)
Risk Factors
Increasing age is the most important risk factor for most cancers. Other risk factors for colorectal cancer include the following:
• Family history of colorectal cancer in a first-degree relative.
• Personal history of colorectal adenomas, colorectal cancer, or ovarian cancer.
• Hereditary conditions, including familial adenomatous polyposis (FAP) and Lynch syndrome (hereditary nonpolyposis colorectal cancer [HNPCC]).
• Personal history of long-standing chronic ulcerative colitis or Crohn colitis.
• Excessive alcohol use.
• Cigarette smoking.
• Race/ethnicity: African American.
• Obesity.
Screening
Because of the frequency of the disease, ability to identify high-risk groups, slow growth of primary lesions, better survival of patients with early-stage lesions, and relative simplicity and accuracy of screening tests, screening for colon cancer should be a part of routine care for all adults aged 50 years and older, especially for those with first-degree relatives with colorectal cancer. (Refer to the PDQ summary on Colorectal Cancer Screening for more information.)
Prognostic Factors
The prognosis of patients with colon cancer is clearly related to the following:
• The degree of penetration of the tumor through the bowel wall.
• The presence or absence of nodal involvement.
• The presence or absence of distant metastases.
These three characteristics form the basis for all staging systems developed for this disease.
Other prognostic factors include the following:
• Bowel obstruction and bowel perforation are indicators of poor prognosis.
• Elevated pretreatment serum levels of carcinoembryonic antigen (CEA) have a negative prognostic significance.
Many other prognostic markers have been evaluated retrospectively for patients with colon cancer, though most, including allelic loss of chromosome 18q or thymidylate synthase expression, have not been prospectively validated. Microsatellite instability, also associated with HNPCC, has been associated with improved survival independent of tumor stage in a population-based series of 607 patients younger than 50 years with colorectal cancer. Patients with HNPCC reportedly have better prognoses in stage-stratified survival analysis than patients with sporadic colorectal cancer, but the retrospective nature of the studies and possibility of selection factors make this observation difficult to interpret.
Treatment decisions depend on factors such as physician and patient preferences and the stage of the disease, rather than the age of the patient.
Racial differences in overall survival (OS) after adjuvant therapy have been observed, without differences in disease-free survival, suggesting that comorbid conditions play a role in survival outcome in different patient populations.
Follow-up and Survivorship
Limited data and no level 1 evidence are available to guide patients and physicians about surveillance and management of patients after surgical resection and adjuvant therapy. The American Society of Clinical Oncology and the National Comprehensive Cancer Network recommend specific surveillance and follow-up strategies.
Following treatment of colon cancer, periodic evaluations may lead to the earlier identification and management of recurrent disease. The impact of such monitoring on overall mortality of patients with recurrent colon cancer, however, is limited by the relatively small proportion of patients in whom localized, potentially curable metastases are found. To date, no large-scale randomized trials have documented an OS benefit for standard, postoperative monitoring programs.
CEA is a serum glycoprotein frequently used in the management of patients with colon cancer. A review of the use of this tumor marker suggests the following:
• A CEA level is not a valuable screening test for colorectal cancer because of the large numbers of false-positive and false-negative reports.
• Postoperative CEA testing should be restricted to patients who would be candidates for resection of liver or lung metastases.
• Routine use of CEA levels alone for monitoring response to treatment should not be recommended.
The optimal regimen and frequency of follow-up examinations are not well defined because the impact on patient survival is not clear and the quality of data is poor.
Factors Associated with Recurrence
Diet and exercise
No prospective randomized trials have demonstrated an improvement in outcome with a specific diet or exercise regimen; however, cohort studies suggest that diet or exercise regimen may improve outcome. The cohort studies contain multiple opportunities for unintended bias, and caution is needed when using the data from them.
Two prospective observational studies were performed with patients enrolled on the Cancer and Leukemia Group B (CALGB-89803 [NCT00003835] trial), which was an adjuvant chemotherapy trial for patients with stage III colon cancer. In this trial, patients in the lowest quintile of the Western dietary pattern compared with those patients in the highest quintile experienced an adjusted hazard ratio (HR) for disease-free survival of 3.25 (95% confidence interval [CI], 2.04–5.19; P < .001) and an OS of 2.32 (95% CI, 1.36–3.96; P < .001). Additionally, findings included that stage III colon cancer patients in the highest quintile of dietary glycemic load experienced an adjusted HR for OS of 1.76 (95% CI, 1.22–2.54; P < .001) compared with those in the lowest quintile. Subsequently, in the Cancer Prevention Study II Nutrition Cohort, among 2,315 participants diagnosed with colorectal cancer, the degree of red and processed meat intake before diagnosis was associated with a higher risk of death (relative risk [RR], 1.29; 95% CI, 1.05–1.59; P = .03), but red meat consumption after diagnosis was not associated with overall mortality.[Level of evidence: 3iiA]
A meta-analysis of seven prospective cohort studies evaluating physical activity before and after a diagnosis of colorectal cancer demonstrated that patients who participated in any amount of physical activity before diagnosis had a RR of 0.75 (95% CI, 0.65–0.87; P < .001) for colorectal cancer-specific mortality compared with patients who did not participate in any physical activity. Patients who participated in a high amount of physical activity (vs. a low amount) before diagnosis had a RR of 0.70 (95% CI, 0.56–0.87; P = .002). Patients who participated in any physical activity (compared with no activity) after diagnosis had a RR of 0.74 (95% CI, 0.58–0.95; P = .02) for colorectal cancer-specific mortality. Those who participated in a high amount of physical activity (vs. a low amount) after diagnosis had a RR of 0.65 (95% CI, 0.47–0.92; P = .01).[Level of evidence: 3iiB]
Aspirin
A prospective cohort study examined the use of aspirin after a colorectal cancer diagnosis. Regular users of aspirin after a diagnosis of colorectal cancer experienced an HR of colon cancer-specific survival of 0.71 (95% CI, 0.65–0.97) and an OS of 0.79 (95% CI, 0.65–0.97).[Level of evidence: 3iiA] One study evaluated 964 patients with rectal or colon cancer from the Nurse’s Health Study and the Health Professionals Follow-up Study. Among patients with PI3K-mutant colorectal cancer, regular use of aspirin was associated with an HR for OS of 0.54 (95% CI, 0.31–0.94; P = .01)[Level of evidence: 3iiiA]
Cellular Classification of Colon Cancer
Histologic types of colon cancer include the following:
• Adenocarcinoma (most colon cancers).
Mucinous (colloid) adenocarcinoma.
Signet ring adenocarcinoma.
• Scirrhous tumors.
• Neuroendocrine. Tumors with neuroendocrine differentiation typically have a poorer prognosis than pure adenocarcinoma variants.
Stage Information for Colon Cancer
Treatment decisions should be made with reference to the TNM (tumor, node, metastasis) classification rather than to the older Dukes or the Modified Astler-Coller classification schema.
The AJCC and a National Cancer Institute–sponsored panel recommended that at least 12 lymph nodes be examined in patients with colon and rectal cancer to confirm the absence of nodal involvement by tumor. This recommendation takes into consideration that the number of lymph nodes examined is a reflection of the aggressiveness of lymphovascular mesenteric dissection at the time of surgical resection and the pathologic identification of nodes in the specimen. Retrospective studies demonstrated that the number of lymph nodes examined in colon and rectal surgery may be associated with patient outcome.
AJCC TNM Definitions
The AJCC has designated staging by TNM classification to define colon cancer. The same classification is used for both clinical and pathologic staging.
cTNM is the clinical classification, and pTNM is the pathologic classification. The y prefix is used for those cancers that are classified after neoadjuvant pretreatment (e.g., ypTNM). Patients who have a complete pathologic response (ypT0, N0, cM0) may be similar to stage group 0 or I. The r prefix is to be used for those cancers that have recurred after a disease-free interval (rTNM).
Primary Tumor (T)
TX = Primary tumor cannot be assessed.
T0 = No evidence of primary tumor.
Tis = Carcinoma in situ: intraepithelial or invasion of lamina propria.
T1 = Tumor invades submucosa.
T2 = Tumor invades muscularis propria.
T3 = Tumor invades through the muscularis propria into pericolorectal tissues.
T4a = Tumor penetrates to the surface of the visceral peritoneum.
T4b = Tumor directly invades or is adherent to other organs or structures.
Note: A satellite peritumoral nodule in the pericolorectal adipose tissue of a primary carcinoma without histologic evidence of residual lymph node in the nodule may represent discontinuous spread, venous invasion with extravascular spread (V1/2), or a totally replaced lymph node (N1/2). Replaced nodes should be counted separately as positive nodes in the N category, whereas discontinuous spread or venous invasion should be classified and counted in the site-specific factor category Tumor Deposits.
Tis includes cancer cells confined within the glandular basement membrane (intraepithelial) or mucosal lamina propria (intramucosal) with no extension through the muscularis mucosae into the submucosa.
Direct invasion in T4 (T4a and T4b) includes invasion of other organs or other segments of the colorectum as a result of direct extension through the serosa, as confirmed on microscopic examination (e.g., invasion of the sigmoid colon by a carcinoma of the cecum) or, for cancers in a retroperitoneal or subperitoneal location, direct invasion of other organs or structures by virtue of extension beyond the muscularis propria (i.e., respectively, a tumor on the posterior wall of the descending colon invading the left kidney or lateral abdominal wall; or a mid or distal rectal cancer with invasion of prostate, seminal vesicles, cervix, or vagina).
Tumor that is adherent to other organs or structures, grossly, is classified cT4b. However, if no tumor is present in the adhesion, microscopically, the classification should be pT1–4a depending on the anatomical depth of wall invasion. The V and L classifications should be used to identify the presence or absence of vascular or lymphatic invasion whereas the PN site-specific factor should be used for perineural invasion.
Regional Lymph Nodes (N)
NX = Regional lymph nodes cannot be assessed.
N0 = No regional lymph node metastasis.
N1 = Metastases in 1–3 regional lymph nodes.
N1a = Metastasis in 1 regional lymph node.
N1b = Metastases in 2–3 regional lymph nodes.
N1c = Tumor deposit(s) in the subserosa, mesentery, or nonperitonealized pericolic or perirectal tissues without regional nodal metastasis.
N2 = Metastases in ≥4 regional lymph nodes.
N2a = Metastases in 4–6 regional lymph nodes.
N2b = Metastases in ≥7 regional lymph nodes.
Distant Metastases (M)
M0 = No distant metastasis.
M1a = Metastasis confined to 1 organ or site (e.g., liver, lung, ovary, nonregional node).
M1b = Metastases in >1 organ/site or the peritoneum.
| Stage | TNM | Dukes | MAC |
| 0 | T1s, N0, M0 | - | - |
| I | T1, N0, M0 | A | A |
| T2, N0, M0 | A | B1 | |
| IIA | T3, N0, M0 | B | B2 |
| IIB | T4a, N0, M0 | B | B2 |
| IIC | T4b, N0, M0 | B | B3 |
| IIIA | T1–T2, N1/N1c, M0 | C | C1 |
| T1, N2a, M0 | C | C1 | |
| IIIB | T3–T4a, N1/N1c, M0 | C | C2 |
| T2–T3, N2a, M0 | C | C1/C2 | |
| T1–T2, N2b, M0 | C | C1 | |
| IIIC | T4a, N2a, M0 | C | C2 |
| T3–T4a, N2b, M0 | C | C2 | |
| T4b, N1–N2, M0 | C | C3 | |
| IVA | Any T, Any N, M1a | - | - |
| IVB | Any T, Any N, M1b | - | - |
Dukes B is a composite of better (T3, N0, M0) and worse (T4, N0, M0) prognostic groups,
as is Dukes C (any T, N1, M0 and any T, N2, M0).
MAC is the modified Astler-Coller classification.
Colon Cancer - Treatment Options
Treatment Options for Colon Cancer
Standard Treatment Options for Stages 0–III Colon Cancer
Stage 0 Colon Cancer
Surgery
Stage I Colon Cancer
Surgery
Stage II Colon Cancer
Surgery
Stage III Colon Cancer
Surgery
Adjuvant chemotherapy
Treatment Options for Stage IV and Recurrent Colon Cancer
Treatment of Liver Metastasis
Surgery
Neoadjuvant chemotherapy
Local ablation
Adjuvant chemotherapy
Intra-arterial chemotherapy
Treatment of Stage IV and Recurrent Colon Cancer
Surgery
Chemotherapy and targeted therapyPrimary Surgical Therapy
Primary Surgical Therapy
Standard treatment for patients with colon cancer has been open surgical resection of the primary and regional lymph nodes for localized disease.
The role of laparoscopic techniques in the treatment of colon cancer has been examined in two studies.
Evidence (laparoscopic techniques):
1. A multicenter, prospective, randomized, noninferiority trial (NCCTG-934653 [NCT00002575]) compared laparoscopic-assisted colectomy (LAC) with open colectomy in 872 patients.
◦At a median follow-up of 4.4 years, 3-year recurrence rates (16% LAC vs. 18% open colectomy; hazard ratio [HR] for recurrence, 0.86; 95% confidence interval [CI], 0.63–1.17; P = .32) and 3-year overall survival (OS) rates (86% LAC vs. 85% open colectomy; HRdeath in LAC, 0.91; 95% CI, 0.68–1.21; P = .51) were similar in both groups for all stages of disease evaluated. Tumor recurrence in surgical incisions was less than 1% for both groups.[Level of evidence: 1iiA]
◦Decreased hospital stay (5 days LAC vs. 6 days open colectomy, P < .001) and decreased use of analgesics were reported in the LAC group. A 21% conversion rate from LAC to open procedure was shown.
◦ This study excluded patients with locally advanced disease, transverse colon and rectal tumor locations, and perforated lesions. Each of the 66 surgeons participating in the trial had performed at least 20 LACs and were accredited for study participation after independent videotape review assured appropriate oncologic and surgical principles were maintained. The quality-of-life component of this trial was published separately and minimal short-term quality-of-life benefits with LAC were reported.[Level of evidence: 1iiC]
2. One small, single-institution randomized study of 219 patients showed that the LAC procedure was independently associated with reduced tumor recurrence on multivariate analysis.Level of evidence: 1iiB]
Surgery is curative in 25% to 40% of highly selected patients who develop resectable metastases in the liver and lung. Improved surgical techniques and advances in preoperative imaging have allowed for better patient selection for resection.
Adjuvant Chemotherapy
The potential value of adjuvant chemotherapy for patients with stage II colon cancer is controversial. Pooled analyses and meta-analyses have suggested a 2% to 4% improvement in OS for patients treated with adjuvant fluorouracil (5-FU)–based therapy compared with observation. (Refer to the Stage II Colon Cancer Treatment section of this summary for more information.)
Prior to 2000, 5-FU was the only useful cytotoxic chemotherapy in the adjuvant setting for patients with stage III colon cancer. Since 2000, capecitabine has been established as an equivalent alternative to 5-FU and leucovorin (5-FU/LV). The addition of oxaliplatin to 5-FU/LV has been shown to improve OS compared with 5-FU/LV alone. (Refer to the Stage III Colon Cancer Treatment section of this summary for more information.)
Adjuvant Radiation Therapy
While combined modality therapy with chemotherapy and radiation therapy has a significant role in the management of patients with rectal cancer (below the peritoneal reflection), the role of adjuvant radiation therapy for patients with colon cancer (above the peritoneal reflection) is not well defined. Patterns-of-care analyses and single-institution retrospective reviews suggest a role for radiation therapy in certain high-risk subsets of colon cancer patients (e.g., T4, tumor location in immobile sites, local perforation, obstruction, and residual disease postresection).
Evidence (adjuvant radiation therapy):
1. Such observations led to the development of a phase III randomized intergroup study designed to test the benefit of adding radiation therapy to surgery and chemotherapy with 5-FU-levamisole for selected high-risk colon cancer patients (e.g., T4; or T3, N1–N2 ascending and/or descending colon).
◦ This clinical trial closed early secondary to inadequate patient accrual, and analysis of 222 enrolled patients (the original goal was 700 patients) demonstrated no relapse or OS benefit for the group receiving radiation therapy, although the sample size
statistical power were inadequate to exclude benefit.
Adjuvant radiation therapy has no current standard role in the management of patients with colon cancer following curative resection, although it may have a role for patients with residual disease.
Chemotherapy regimens
| Regimen Name | Drug Combinations |
Dose |
| AIO or German AIO |
Folic acid, 5-FU, and irinotecan |
Irinotecan (100 mg/m2) and LV (500 mg/m2) administered as 2-hour infusions on d 1, followed by 5-FU (2,000 mg/m2) IV bolus administered via ambulatory pump weekly over 24 h, 4 times a y (52 wk). |
| CAPOX | Capecitabine and oxaliplatin |
Capecitabine (1,000 mg/m2) bid on d 1–14, plus oxaliplatin (70 mg/m2) on d 1 and 8 every 3 wk. |
| Douillard | Folic acid, 5-FU, and irinotecan |
Irinotecan (180 mg/m2) administered as a 2-h infusion on d 1, LV (200 mg/m2) administered as a 2-h infusion on d 1 and 2, followed by a loading dose of 5-FU (400 mg/m2) IV bolus, then 5-FU (600 mg/m2) administered via ambulatory pump over 22 h every 2 wk on d 1 and 2. |
| FOLFIRI | LV, 5-FU, and irinotecan |
Irinotecan (180 mg/m2) and LV (400 mg/m2) administered as 2-h infusions on d 1, followed by a loading dose of 5-FU (400 mg/m2) IV bolus administered on d 1, then 5-FU (2,400–3,000 mg/m2) administered via ambulatory pump over 46 h every 2 wk. |
| FOLFOX-4 | Oxaliplatin, LV, and 5-FU |
Oxaliplatin (85 mg/m2) administered as a 2-h infusion on d 1, LV (200 mg/m2) administered as a 2-h infusion on d 1 and 2, followed by a loading dose of 5-FU (400 mg/m2) IV bolus, then 5-FU (600 mg/m2) administered via ambulatory pump over 22 h every 2 wk on d 1 and 2. |
| FOLFOX-6 | Oxaliplatin, LV, and 5-FU |
Oxaliplatin (85–100 mg/m2) and LV (400 mg/m2) administered as 2-h infusions on d 1, followed by a loading dose of 5-FU (400 mg/m2) IV bolus on d 1, then 5-FU (2,400–3,000 mg/m2) administered via ambulatory pump over 46 h every 2 wk. |
| FOLFOXIRI | Irinotecan, oxaliplatin, LV, and 5-FU |
Irinotecan (165 mg/m2) administered as a 60-min infusion, then concomitant infusion of oxaliplatin (85 mg/m2) and LV (200 mg/m2) over 120 min, followed by 5-FU (3,200 mg/m2) administered as a 48-h continuous infusion. |
| FUFOX | 5-FU, LV, and oxaliplatin |
Oxaliplatin (50 mg/m2) plus LV (500 mg/m2) plus 5-FU (2,000 mg/m2) administered as a 22-h continuous infusion on d 1, 8, 22, and 29 every 36 d. |
| FUOX | 5-FU plus oxaliplatin |
5-FU (2,250 mg/m2) administered as a continuous infusion over 48 h on d 1, 8, 15, 22, 29, and 36 plus oxaliplatin (85 mg/m2) on d 1, 15, and 29 every 6 wk. |
| IFL (or Saltz) | Irinotecan, 5-FU, and LV |
Irinotecan (125 mg/m2) plus 5-FU (500 mg/m2) IV bolus and LV (20 mg/m2) IV bolus administered weekly for 4 out of 6 wk. |
| XELOX | Capecitabine plus oxaliplatin |
Oral capecitabine (1,000 mg/m2) administered bid for 14 d plus oxaliplatin (130 mg/m2) on d 1 every 3 wk. |
FOL: folinic acid (leucovorin), F: flurouracil, OX: oxaliplatin, IRI: irinotecan
AIO = Arbeitsgemeinschaft Internistische Onkologie; LV = leucovorin.
Stage 0 Colon Cancer Treatment
Stage 0 colon cancer is the most superficial of all the lesions and is limited to the mucosa without invasion of the lamina propria. Because of its superficial nature, the surgical procedure may be limited.
Standard Treatment Options for Stage 0 Colon Cancer
Surgery
1. Local excision or simple polypectomy with clear margins.
2. Colon resection for larger lesions not amenable to local excision.
Stage I Colon Cancer Treatment
Because of its localized nature, stage I colon cancer has a high cure rate.
Standard Treatment Options for Stage I Colon Cancer
Surgery
1. Wide surgical resection and anastomosis.
Evidence (laparoscopic techniques):
The role of laparoscopic techniques in the treatment of colon cancer was examined in a multicenter, prospective, randomized trial (NCCTG-934653 [NCT00002575]) comparing laparoscopic-assisted colectomy (LAC) with open colectomy.
• Three-year recurrence rates and 3-year overall survival rates were similar in the two groups. (Refer to the Primary Surgical Therapy section in the Treatment Option Overview section of this summary for more information.)
• The quality-of-life component of this trial has been published and minimal short-term quality-of-life benefits with LAC were reported.[Level of evidence: 1iiC]
Stage II Colon Cancer Treatment
Standard Treatment Options for Stage II Colon Cancer
Surgery
1. Wide surgical resection and anastomosis.
Evidence (laparoscopic techniques):
The role of laparoscopic techniques in the treatment of colon cancer was examined in a multicenter, prospective, randomized trial (NCCTG-934653 [NCT00002575]) comparing laparoscopic-assisted colectomy (LAC) to open colectomy.
• Three-year recurrence rates and 3-year overall survival (OS) rates were similar in the two groups. (Refer to the Primary Surgical Therapy section in the Treatment Option Overview section of this summary for more information.)
• The quality-of-life component of this trial has been published and minimal short-term quality-of-life benefits with LAC were reported.[Level of evidence: 1iiC]
Treatment Options Under Clinical Evaluation
Adjuvant chemotherapy
The potential value of adjuvant chemotherapy for patients with stage II colon cancer remains controversial. Although subgroups of patients with stage II colon cancer may be at higher-than-average risk for recurrence (including those with anatomic features such as tumor adherence to adjacent structures, perforation, and complete obstruction), evidence is inconsistent that adjuvant 5-fluorouracil (5-FU)–based chemotherapy is associated with an improved OS compared with surgery alone.
Features in patients with stage II colon cancer that are associated with an increased risk of recurrence include the following:
• Inadequate lymph node sampling.
• T4 disease.
• Involvement of the visceral peritoneum.
• A poorly differentiated histology.
The decision to use adjuvant chemotherapy for patients with stage II colon cancer is complicated and requires thoughtful consideration by both patients and their physicians. Adjuvant therapy is not indicated for most patients unless they are entered into a clinical trial.
Evidence (adjuvant chemotherapy):
1. The GRECCR-03 (NCT00046995) and NCRI-QUASAR1 (NCT00005586) trials evaluated the use of systemic or regional chemotherapy or biologic therapy. Following surgery, patients should be considered for entry into a carefully controlled clinical trial.
2. Investigators from the National Surgical Adjuvant Breast and Bowel Project have indicated that the reduction in risk of recurrence by adjuvant therapy in patients with stage II disease is of similar magnitude to the benefit seen in patients with stage III disease treated with adjuvant therapy, though an OS advantage has not been established.
3. A meta-analysis of 1,000 stage II patients whose experience was amalgamated from a series of trials indicates a 2% advantage in disease-free survival at 5 years when adjuvant therapy–treated patients treated with 5-FU/leucovorin are compared with untreated controls.[Level of evidence: 1iiDii];
4. The Cancer Care Ontario Practice Guideline Initiative Gastrointestinal Cancer Disease Site Group undertook a meta-analysis of the English language–published literature consisting of randomized trials in which adjuvant chemotherapy was compared with observation for patients with stage II colon cancer. ◦
The mortality risk ratio was 0.87 (95% confidence interval, 0.75–1.01; P = .07).
Based on these data, the American Society of Clinical Oncology issued a guideline stating “direct evidence from randomized controlled trials does not support the routine use of adjuvant chemotherapy for patients with stage II colon cancer.”
Stage III Colon Cancer Treatment
Stage III colon cancer denotes lymph node involvement. Studies have indicated that the number of lymph nodes involved affects prognosis; patients with one to three involved nodes have a significantly better survival than those with four or more involved nodes.
Standard Treatment Options for Stage III Colon Cancer
1. Surgery.
2. Adjuvant chemotherapy.
Surgery
Surgery for stage III colon cancer is wide surgical resection and anastomosis.
Evidence (laparoscopic techniques):
The role of laparoscopic techniques in the treatment of colon cancer was examined in a multicenter, prospective, randomized trial (NCCTG-934653 [NCT00002575]) comparing laparoscopic-assisted colectomy (LAC) with open colectomy.
• Three-year recurrence rates and 3-year overall survival (OS) rates were similar in the two groups. (Refer to the Primary Surgical Therapy section in the Treatment Option Overview section of this summary for more information.)
• The quality-of-life component of this trial has been published and minimal short-term quality-of-life benefits with LAC were reported.[Level of evidence: 1iiC]
Adjuvant chemotherapy
Chemotherapy regimens prior to 2000
Prior to 2000, 5-fluorouracil (5-FU) was the only useful cytotoxic chemotherapy in the adjuvant setting for patients with stage III colon cancer. Many of the early randomized studies of 5-FU in the adjuvant setting failed to show a significant improvement in survival for patients. These trials employed 5-FU alone or 5-FU/semustine.
Evidence (5-FU alone and 5-FU/semustine):
1. The North Central Cancer Treatment Group conducted a randomized trial comparing surgical resection alone with postoperative levamisole or levamisole/5-FU.[Level of evidence: 1iiA]
◦ A significant improvement in disease-free survival (DFS) was observed for patients with stage III colon cancer who received levamisole/5-FU, but OS benefits were of borderline statistical significance.
◦ An absolute survival benefit of approximately 12% (49% vs. 37%) was seen in patients with stage III disease treated with levamisole/5-FU.
2. In a large confirmatory intergroup trial, levamisole/5-FU- prolonged DFS and OS in patients with stage III colon cancer compared with patients who received no treatment after surgery.[Level of evidence: 1iiA] Levamisole alone did not confer these benefits.
3. Subsequent studies tested the combination of 5-FU/leucovorin (5-FU/LV) in the adjuvant treatment of patients with resected carcinoma of the colon.
◦ Results of multiple randomized trials that have enrolled more than 4,000 patients comparing adjuvant chemotherapy with 5-FU/LV to surgery or 5-FU/semustine/vincristine demonstrate a relative reduction in mortality of between 22% and 33% (3-year OS of 71%–78% increased to 75%–84%).
4. The completed Intergroup trial 0089 (INT-0089 [NCT00201331]) randomly assigned 3,794 patients with high-risk stage II or stage III colon cancer to one of the following four treatment arms:
◦ The Mayo Clinic regimen administered for a total of six cycles.
◦ The Roswell Park regimen administered for a total of four cycles.
◦ The Mayo Clinic regimen administered with levamisole for six cycles.
◦ The levamisole regimen administered for a total of 1 year.
Results:
◦ Five-year OS ranged from 49% for the Mayo Clinic regimen with levamisole to 60% for the Mayo Clinic regimen, and there were no statistically significant differences among treatment arms.[Level of evidence: 1iiA]
◦ A preliminary report in November 1997 demonstrated a statistically significant advantage for OS for the Mayo Clinic regimen with levamisole compared with the levamisole regimen. This difference became insignificant with longer follow-up.
◦ Overall, grade 3 or greater toxicity occurred more frequently for the Mayo Clinic regimen and the Mayo Clinic regimen with levamisole. In addition, the Mayo Clinic regimen was significantly more toxic with levamisole than without levamisole.
◦ The death rate for all four regimens ranged from 0.5% to 1%.
◦ Because of its ease of use and its good toxicity profile, the Roswell Park regimen became the preferred adjuvant regimen used in the United States and was often the control arm in subsequent randomized studies.
5. In addition to INT-0089, multiple studies have refined the use of 5-FU/LV in the adjuvant setting and can be summarized as follows:
◦ Levamisole is unnecessary when using leucovorin.
◦ Treatment that includes 6 to 8 months of 5-FU/LV is equivalent to 12 months of therapy.
◦ Treatment that includes 24 weeks of adjuvant 5-FU/LV is equivalent to 36 weeks of therapy.
◦ High-dose leucovorin is equivalent to low-dose leucovorin.
◦ A meta-analysis of seven trials revealed no significant difference in efficacy or toxicity among patients 70 years or younger compared with patients older than 70 years.
◦ An infusional deGramont bolus and infusional 5-FU/LV schedule is safer than a bolus modified Mayo Clinic schedule of 5-FU/LV.
Chemotherapy regimens after 2000
(Note: Only fluoropyrimidine and oxaliplatin have curative potential in the adjuvant setting.)
■ Capecitabine
Capecitabine is an oral fluoropyrimidine that undergoes a three-step enzymatic conversion to 5-FU with the last step occurring in the tumor cell. For patients with metastatic colon cancer, two studies have demonstrated the equivalence of capecitabine to 5-FU/LV.
For patients with stage III colon cancer, capecitabine provides equivalent outcome to intravenous 5-FU/LV.
Evidence (capecitabine):
1. A multicenter European study compared capecitabine (1,250 mg/m2) administered twice daily for days 1 to 14, then given every 21 days for eight cycles against the Mayo Clinic schedule of 5-FU and low-dose LV for patients with stage III colon cancer.
- The study demonstrated that DFS at 3 years is equivalent for patients who received capecitabine or 5-FU/LV (hazard ratio [HR], 0.87; P < .001).[Level of evidence: 1iiDii]
- Hand-foot syndrome and hyperbilirubinemia were significantly more common for patients receiving capecitabine, but diarrhea, nausea or vomiting, stomatitis, alopecia, and neutropenia were significantly less common.
- Of patients receiving capecitabine, 57% required a dose modification.
- For patients with stage III colon cancer in whom treatment with 5-FU/LV is planned, capecitabine is an equivalent alternative.
■ Oxaliplatin
Oxaliplatin has significant activity when combined with 5-FU/LV in patients with metastatic colorectal cancer.
Evidence (oxaliplatin):
1. In the 2,246 patients with resected stage II or stage III colon cancer in the completed Multicenter International Study of Oxaliplatin/5-Fluorouracil/Leucovorin in the Adjuvant Treatment of Colon Cancer (MOSAIC [NCT00275210]) study, the toxic effects and efficacy of FOLFOX-4 (oxaliplatin/LV/5-FU) were compared with the same 5-FU/LV regimen without oxaliplatin administered for 6 months.
Based on results from the MOSAIC trial, adjuvant FOLFOX-4 demonstrated prolonged OS for patients with stage III colon cancer compared with patients receiving 5-FU/LV without oxaliplatin.
◦ The preliminary results of the study with 37 months of follow-up demonstrated a significant improvement in DFS at 3 years (77.8% vs. 72.9%; P = .01) in favor of FOLFOX-4. When initially reported, there was no difference in OS.[Level of evidence: 1iiDii]
◦ Further follow-up at 6 years demonstrated that the OS for all patients (both stage II and stage III) entered into the study was not significantly different (OS = 78.5% vs. 76.0%; HR, 0.84; 95% confidence interval [CI], 0.71–1.00).
On subset analysis, the 6-year OS in patients with stage III colon cancer was 72.9% in the patients receiving FOLFOX-4 and 68.7% in the patients receiving 5-FU/LV (HR, 0.80; 95% CI, 0.65–0.97; P = .023).[Level of evidence: 1iiA]
◦ Patients treated with FOLFOX-4 experienced more frequent toxic effects consisting mainly of neutropenia (41% >grade 3) and reversible peripheral sensorial neuropathy (12.4% >grade 3).
FOLFOX has become the reference standard for the next generation of clinical trials for patients with stage III colon cancer.
Treatment Options Under Clinical Evaluation
Eligible patients should be considered for entry into carefully controlled clinical trials comparing various postoperative chemotherapy regimens.
Stage IV and Recurrent Colon Cancer Treatment
Stage IV colon cancer denotes distant metastatic disease. Treatment of recurrent colon cancer depends on the sites of recurrent disease demonstrable by physical examination and/or radiographic studies. In addition to standard radiographic procedures, radioimmunoscintography may add clinical information that may affect management. Such approaches have not led to improvements in long-term outcome measures such as survival.
Treatment Options for Stage IV and Recurrent Colon Cancer
1. Surgical resection of locally recurrent cancer.
2. Surgical resection and anastomosis or bypass of obstructing or bleeding primary lesions in selected metastatic cases.
3. Resection of liver metastases in selected metastatic patients (5-year cure rate for resection of solitary or combination metastases exceeds 20%) or ablation in selected patients.
4. Resection of isolated pulmonary or ovarian metastases in selected patients.
5. Palliative radiation therapy.
6. Palliative chemotherapy.
7. Targeted therapy.
8. Clinical trials evaluating new drugs and biological therapy.
9. Clinical trials comparing various chemotherapy regimens or biological therapy, alone or in combination.
Treatment of Liver Metastasis
Approximately 50% of colon cancer patients will be diagnosed with hepatic metastases, either at the time of initial presentation or as a result of disease recurrence.
Although only a small proportion of patients with hepatic metastases are candidates for surgical resection, advances in tumor ablation techniques and in both regional and systemic chemotherapy administration provide for a number of treatment options. These include the following:
• Surgery.
• Neoadjuvant chemotherapy.
• Local ablation.
• Adjuvant chemotherapy.
• Intra-arterial chemotherapy.
Surgery
Hepatic metastasis may be considered to be resectable based on the following:
• Limited number of lesions.
• Intrahepatic locations of lesions.
• Lack of major vascular involvement.
• Absent or limited extrahepatic disease.
• Sufficient functional hepatic reserve.
For patients with hepatic metastasis that is considered to be resectable, a negative margin resection resulted in 5-year survival rates of 25% to 40% in mostly nonrandomized studies. Improved surgical techniques and advances in preoperative imaging have allowed for better patient selection for resection. In addition, multiple studies with multiagent chemotherapy have demonstrated that patients with metastatic disease isolated to the liver, which historically would be considered unresectable, can occasionally be made resectable after the administration of chemotherapy.
Neoadjuvant chemotherapy for unresectable liver metastases
Patients with hepatic metastases that are deemed unresectable will occasionally become candidates for resection if they have a good response to chemotherapy. These patients have 5-year survival rates similar to patients who initially had resectable disease. There is no consensus on the best regimen to use to convert unresectable isolated liver metastases to resectable liver metastases.
Local ablation
Radiofrequency ablation has emerged as a safe technique (2% major morbidity and <1% mortality rate) that may provide for long-term tumor control. Radiofrequency ablation and cryosurgical ablation remain options for patients with tumors that cannot be resected and for patients who are not candidates for liver resection.
Other local ablative techniques that have been used to manage liver metastases include embolization and interstitial radiation therapy. Patients with limited pulmonary metastases, and patients with both pulmonary and hepatic metastases, may also be considered for surgical resection, with 5-year survival possible in highly-selected patients.
Adjuvant or neoadjuvant chemotherapy for resectable liver metastases
The role of adjuvant chemotherapy after potentially curative resection of liver metastases is uncertain.
Evidence (adjuvant or neoadjuvant chemotherapy for resectable liver metastases):
In the era before the use of FOLFOX (folinic acid [LV], 5-fluorouracil [5-FU], and oxaliplatin) and FOLFIRI (5-FU/leucovorin [LV]/irinotecan), two trials attempted to randomly assign patients after resection of liver metastases to 5-FU/ or observation, but both studies were closed early because of poor accrual.
1. The FFCD-9902 [NCT00304135] trial randomly assigned 173 patients (200 patients were planned) to postoperative 5-FU/LV, which is the Mayo Clinic regimen, or observation.
◦ The 5-year disease-free survival (DFS) rate was 33.5% for patients in the chemotherapy group and 26.7% for patients in the control group (Cox multivariate analysis: odds ratio (OR) for recurrence or death, 0.66; 95% confidence interval [CI], 0.46–0.96; P = .028). The 5-year overall survival (OS) was not significantly different between the groups (chemotherapy group, 51.1% vs. the control group, 41.1%; ORdeath, 0.73; 95% CI, 0.48–1.10; P = .13).
2. The European Organization for Research and Treatment of Cancer/National Cancer Institute of Canada/Gruppo Interdisciplinare Valutazione Interventi in Oncologia (EORTC/NCIC/GIVIO) International trial attempted a similar random assignment of patients after surgical resection of liver metastases. The study closed because of poor accrual, and a combined analysis of the study and the FFCD-9902 study was done instead. In the combined analysis, 278 patients (138 of whom received chemotherapy; 14 of whom received surgery alone) were included.
◦ Median progression-free survival (PFS) was 27.9 months in the chemotherapy arm and 18.8 months in the surgery alone arm (hazard ratio [HR], 1.32; 95% CI, 1.00–1.76; P = .058).
◦ Median OS was 62.2 months in the chemotherapy arm compared with 47.3 months in the surgery-alone arm (HR, 1.32; 95% CI, 0.95–1.82; P = .095).
In the era of multiagent chemotherapy, two subsequent studies evaluated its role in the adjuvant setting following resection of liver metastases from colorectal cancer.
1. A phase III study randomly assigned 306 patients to 5-FU /LV or FOLFIRI after a resection of liver metastases.
◦ There was no difference in DFS (21.6 months for 5-FU/LV vs. 24.7 months for FOLFIRI; HR, 0.89; log-rank P = .44) or OS (HR, 1.09; 95% CI, 0.72–1.64).
2. he EORTC (EORTC-40983 [NCT00006479]) trial randomly assigned 364 patients with up to four resectable liver metastases to perioperative FOLFOX (six cycles presurgery and six cycles postsurgery) or surgery alone.
◦ The PFS was 28.1% (95.66% CI, 21.3–35.5) for the surgery-alone group and 35.4% (28.1–42.7; HR 0.79; 0.62–1.02; P = .058) for the perioperative chemotherapy group. There was no difference in OS. Subsequent post hoc analysis demonstrated that the difference in PFS in truly eligible patients rose 8.1% (from 28.1% [21.2–36.6] to 36.2% [28.7–43.8]; HR, 0.77 [0.60–1.00]; P = .041). In patients who actually underwent resection of liver metastases, the difference in PFS rose 9.2% (from 33.2% [25.3–41.2] to 42.4% [34.0–50.5]; HR, 0.73 [0.55–0.97]; P = .025).
◦ Reversible postoperative complications occurred more often after chemotherapy than after surgery (40 [25%] of the 159 complications vs. 27 [16%] of the 170 complications; P = .04). After surgery, there were two deaths in the surgery-alone group and one in the perioperative chemotherapy group.
There is no level 1 evidence demonstrating that perioperative or postoperative chemotherapy improves OS for patients undergoing resection of liver metastases.
Nevertheless, on the basis of post hoc subset analyses of the EORTC study, some physicians feel perioperative or postoperative therapy is reasonable in this setting.
Intra-arterial chemotherapy after liver resection
Hepatic intra-arterial chemotherapy with floxuridine for liver metastases has produced higher overall response rates but no consistent improvement in survival when compared with systemic chemotherapy. A meta-analysis of the randomized studies, which were all done in the era when only fluoropyrimidines were available for systemic therapy, did not demonstrate a survival advantage.
Evidence (intra-arterial chemotherapy after liver resection):
Two trials evaluated hepatic arterial floxuridine in the adjuvant setting after liver resection.
1. A trial of hepatic arterial floxuridine and dexamethasone plus systemic 5-FU/LV compared with systemic 5-FU/LV alone showed improved 2-year PFS (57% vs. 42%, P = .07) and OS (86% vs. 72%, P = .03) for patients in the combined therapy arm but did not show a significant statistical difference in median survival compared with systemic 5-FU therapy alone.[Level of evidence: 1iiA]
◦ Median survival in the combined therapy arm was 72.2 months versus 59.3 months in the monotherapy arm (P = .21).
2. A second trial preoperatively randomly assigned 109 patients who had one to three potentially resectable colorectal hepatic metastases to either no further therapy or postoperative hepatic arterial floxuridine plus systemic 5-FU. Of those randomly assigned patients, 27% were deemed ineligible at the time of surgery, which left only 75 patients evaluable for recurrence and survival.
◦ While liver cancer recurrence was decreased, median or 4-year survival was not significantly different between the patient groups.
Further studies are required to evaluate this treatment approach and to determine whether more effective systemic combination chemotherapy alone may provide similar results compared with hepatic intra-arterial therapy plus systemic treatment.
Several studies show increased local toxic effects with hepatic infusional therapy, including liver function abnormalities and fatal biliary sclerosis.
Treatment of Stage IV and Recurrent Colon Cancer
• Surgery.
• Chemotherapy and targeted therapy.
Surgery
Treatment of patients with recurrent or advanced colon cancer depends on the location of the disease. For patients with locally recurrent and/or liver-only and/or lung-only metastatic disease, surgical resection, if feasible, is the only potentially curative treatment.
Chemotherapy and targeted therapy
Currently, there are thirteen active U.S. Food and Drug Administration (FDA)-approved drugs for patients with metastatic colorectal cancer that are used alone and in combination with other drugs:
■ 5-FU.
■ Capecitabine.
■ Irinotecan.
■ Oxaliplatin.
■ Bevacizumab.
■ FOLFOXIRI (irinotecan, oxaliplatin, LV, and 5-FU).
■ Cetuximab.
■ Aflibercept.
■ Ramucirumab.
■ Panitumumab.
■ Anti-epidermal growth factor receptor (EGFR) antibody versus anti-vascular endothelial growth factor (VEGF) antibody with first-line chemotherapy.
■ Regorafenib.
■ TAS-102.
■ 5-FU
When 5-FU was the only active chemotherapy drug, trials in patients with locally advanced, unresectable, or metastatic disease demonstrated partial responses and prolongation of the time-to-progression (TTP) of disease, and improved survival and quality of life for patients who received chemotherapy versus best supportive care.
Several trials have analyzed the activity and toxic effects of various 5-FU/LV regimens using different doses and administration schedules and showed essentially equivalent results with a median survival time in the 12-month range.
■ Capecitabine
Before the advent of multiagent chemotherapy, two randomized studies demonstrated that capecitabine was associated with equivalent efficacy when compared with the Mayo Clinic regimen of 5-FU/LV.[Level of evidence: 1iiA]
■ Irinotecan
Three randomized studies demonstrated improved response rates, PFS, and OS when irinotecan or oxaliplatin was combined with 5-FU/LV.
Evidence (irinotecan):
1. An intergroup study (NCCTG-N9741 [NCT00003594]) compared irinotecan/5-FU/LV (IFL) with oxaliplatin/LV/5-FU (FOLFOX-4) in first-line treatment for patients with metastatic colorectal cancer.
◦ Patients assigned to FOLFOX-4 experienced an improved PFS (median, 6.9 months vs. 8.7 months; P = .014; HR, 0.74; 95% confidence interval [CI], 0.61–0.89) and OS (15.0 months vs. 19.5 months, P = .001; HR, 0.66; 95% CI, 0.54–0.82) compared with patients randomly assigned to IFL.
2. Subsequently, two studies compared FOLFOX with FOLFIRI, and patients were allowed to cross over upon progression on first-line therapy, respectively.[Level of evidence: 1iiDiii]
◦ PFS and OS were identical between the treatment arms in both studies.
3. The Bolus, Infusional, or Capecitabine with Camptosar-Celecoxib (BICC-C [NCT00094965]) trial evaluated several different irinotecan-based regimens in patients with previously untreated metastatic colorectal cancer, including FOLFIRI, irinotecan plus bolus 5-FU/LV (mIFL), and capecitabine/irinotecan (CAPIRI).[Level of evidence: 1iiA]
◦ The study randomly assigned 430 patients and was closed early because of poor accrual.
◦ The patients who received FOLFIRI had a better PFS than the patients who received either mIFL (7.6 months vs. 5.9 months, P = .004) or CAPIRI (7.6 months vs. 5.8 months, P = .015).
◦ Patients who received CAPIRI had the highest grade 3 or higher rates of nausea, vomiting, diarrhea, dehydration, and hand-foot syndrome.
Since the publication of these studies, the use of either FOLFOX or FOLFIRI is considered acceptable for first-line treatment of patients with metastatic colorectal cancer.
When using an irinotecan-based regimen as first-line treatment of metastatic colorectal cancer, FOLFIRI is preferred.[Level of evidence: 1iiDiii]
■ Oxaliplatin
Randomized phase III trials have addressed the equivalence of substituting capecitabine for infusional 5-FU. Two phase III studies have evaluated 5-FU/oxaliplatin (FUOX) versus capecitabine/oxaliplatin (CAPOX).
Evidence (oxaliplatin):
1. The AIO Colorectal Study Group randomly assigned 474 patients to either 5-FU/LV/oxaliplatin (FUFOX) or CAPOX.
◦ The median PFS was 7.1 months for the CAPOX arm and 8.0 months for the FUFOX arm (HR, 1.17; 95% CI, 0.96–1.43; P = .117), and the HR was in the prespecified equivalence range.
2. The Spanish Cooperative Group randomly assigned 348 patients to CAPOX or FUOX.]Level of evidence: 1iiDiii
◦ The TTP was 8.9 months versus 9.5 months (P = .153) and met the prespecified range for noninferiority.
When using an oxaliplatin-based regimen as first-line treatment of metastatic colorectal cancer, a CAPOX regimen is not inferior to a FUOX regimen.
Before the availability of cetuximab, panitumumab, bevacizumab, and aflibercept as second-line therapy, second-line chemotherapy with irinotecan in patients treated with 5-FU/LV as first-line therapy demonstrated improved OS when compared with either infusional 5-FU or supportive care.
Similarly, a phase III trial randomly assigned patients who progressed on irinotecan and 5-FU/LV to bolus and infusional 5-FU/LV (LV5FU2), single-agent oxaliplatin, or FOLFOX-4. The median TTP for FOLFOX-4 versus LV5FU2 was 4.6 months versus 2.7 months (stratified log-rank test, 2-sided P < .001).[Level of evidence: 1iiDiii]
■ Bevacizumab
Bevacizumab is a partially humanized monoclonal antibody that binds to VEGF. Bevacizumab can reasonably be added to either FOLFIRI or FOLFOX for patients undergoing first-line treatment of metastatic colorectal cancer.
Evidence (bevacizumab):
1. After bevacizumab was approved, the BICC-C trial was amended, and an additional 117 patients were randomly assigned to receive FOLFIRI/bevacizumab or mIFL/bevacizumab.
◦ Although the primary endpoint of PFS was not significantly different, patients who received FOLFIRI/bevacizumab had a significantly better OS (not yet reached with a median follow-up of 22.6 months vs. 19.2 months, P = .007).
2. Patients with previously untreated metastatic colorectal cancer were randomly assigned to either IFL or IFL/bevacizumab.[Level of evidence: 1iiA]
◦ The patients randomly assigned to IFL/bevacizumab experienced a significantly better PFS (10.6 months in the group given IFL/bevacizumab, as compared with 6.2 months in the group given IFL/placebo; HRdisease progression, 0.54; P < .001) and OS (20.3 months in the group given IFL/ bevacizumab, as compared with 15.6 months in the group given IFL/ and placebo corresponding to an HRdeath , 0.66; P < .001).
3. Despite the lack of direct data, in standard practice, bevacizumab was added to FOLFOX as a standard first-line regimen based on the results of the NCCTG-N9741 trial. Subsequently, in a randomized phase III study, patients with untreated, stage IV, colorectal cancer were randomly assigned in a 2 × 2 factorial design to CAPOX versus FOLFOX-4, then to bevacizumab versus placebo. PFS was the primary endpoint.
◦ In this trial, 1,401 patients were randomly assigned, and the median PFS was 9.4 months for patients receiving bevacizumab and 8.0 months for the patients receiving placebo (HR, 0.83; 97.5% CI, 0.72–0.95; P = .0023).[Level of evidence: 1iiDiii]
◦ Median OS was 21.3 months for patients receiving bevacizumab and 19.9 months for patients receiving placebo (HR, 0.89; 97.5% CI, 0.76–1.03; P = .077).
◦ The median PFS (intention-to-treat analysis) was 8.0 months in the pooled CAPOX-containing arms versus 8.5 months in the FOLFOX-4-containing arms (HR, 1.04; 97.5% CI, 0.93–1.16), with the upper limit of the 97.5% CI being below the predefined noninferiority margin of 1.23.
◦ The effect of bevacizumab on OS is likely to be less than what was seen in the original Hurwitz study.
4. Investigators from the Eastern Cooperative Oncology Group randomly assigned patients who had progressed on 5-FU/leucovorin and irinotecan to either FOLFOX or FOLFOX /bevacizumab.
◦ Patients randomly assigned to FOLFOX and bevacizumab experienced a statistically significant improvement in PFS (7.43 months vs. 4.7 months, HR, 0.61; P < .0001) and OS (12.9 months vs. 10.8 months, HR, 0.75; P = .0011).[Level of evidence: 1iiA]
Based on these studies, bevacizumab can reasonably be added to either FOLFIRI or FOLFOX for patients undergoing first-line treatment of metastatic colorectal cancer.
A major question was whether the use of bevacizumab after first-line therapy was warranted when bevacizumab was used as a component of first-line therapy. At the 2012 American Society of Clinical Oncology (ASCO) Annual Meeting, data were presented from a randomized, controlled trial. In the trial, 820 patients with metastatic colorectal cancer, after progressing on first-line chemotherapy that included bevacizumab, were randomly assigned to chemotherapy without bevacizumab or chemotherapy with bevacizumab. Patients who received bevacizumab experienced an improved OS compared with the patients who did not receive bevacizumab. Median OS was 11.2 months for patients who received bevacizumab/chemotherapy and 9.8 months for patients who received chemotherapy without bevacizumab (HR, 0.81; 95% CI, 0.69–0.94; unstratified log-rank test, P = .0062). Median PFS was 5.7 months for patients who received bevacizumab/chemotherapy and 4.1 months for those who received chemotherapy without bevacizumab (HR, 0.68; 95% CI, 0.59–0.78; unstratified log-rank test, P < .0001). [Level of evidence: 1iiA]
■ FOLFOXIRI
Evidence (FOLFOXIRI):
1. The combination of FOLFOXIRI with bevacizumab was compared with FOLFIRI with bevacizumab in a randomized, phase III study of 508 patients with untreated metastatic colorectal cancer.[Level of evidence: 1iiDiii]
◦ The median PFS was 12.1 months in the FOLFOXIRI group, compared with 9.7 months in the FOLFIRI group (HRprogression, 0.75; 95% CI, 0.62–0.90; P = .003). OS was not significantly different between the groups (31.0 vs. 25.8 months; HRdeath, 0.79; 95% CI, 0.63–1.00; P = .054).
◦ Patients who received FOLFOXIRI had significantly more grade 3 and 4 toxicities, including neutropenia, stomatitis, and peripheral neuropathy.
■ Cetuximab
Cetuximab is a partially humanized monoclonal antibody against the EGFR. Because cetuximab affects tyrosine kinase signaling at the surface of the cell membrane, tumors with mutations causing activation of the pathway downstream of the EGFR, such as KRAS mutations, are not sensitive to its effects.
The addition of cetuximab to multiagent chemotherapy improves survival in patients with colon cancers that lack a KRAS mutation (i.e., KRAS wild type). Importantly, patients with mutant KRAS tumors may experience worse outcome when cetuximab is added to multiagent chemotherapy regimens containing bevacizumab.
Evidence (cetuximab):
1. For patients who have progressed on irinotecan-containing regimens, a randomized, phase II study was performed using either cetuximab or irinotecan and cetuximab.[Level of evidence: 3iiiDiv]
◦ The median TTP for patients who received cetuximab was 1.5 months, compared with the median TTP of 4.2 months for patients receiving irinotecan/cetuximab.[Level of evidence: 1iiDiii]
◦ On the basis of this study, cetuximab was approved for use in patients with metastatic colorectal cancer refractory to 5-FU and irinotecan.
2.The Crystal Study (EMR 62202-013 [NCT00154102]) randomly assigned 1,198 patients with stage IV colorectal cancer to FOLFIRI with or without cetuximab.[Level of evidence: 1iiDii]
◦ The addition of cetuximab was associated with an improved PFS (HR, 0.85; 95% CI, 0.72–0.99; P = .048, by a stratified log rank test) but not OS.
◦ Retrospective studies of patients with metastatic colorectal cancer have suggested that responses to anti-EGFR antibody therapy are confined to patients with tumors that harbor wild types of KRAS (i.e., lack activating mutations at codon 12 or 13 of the KRAS gene).
◦ A subset analysis evaluating efficacy vis-à-vis KRAS status was done in patients enrolled on the Crystal Study. There was a significant interaction for KRAS mutation status and treatment for tumor response (P = .03) but not for PFS (P = .07). Among patients with KRAS wild-type tumors, the HR favored the FOLFIRI/cetuximab group (HR, 0.68; 95% CI, 0.50–0.94).
3. In a randomized trial, patients with metastatic colorectal cancer received capecitabine/oxaliplatin/bevacizumab with or without cetuximab.[Level of evidence: 1iiDiii]
◦ The median PFS was 9.4 months in the group who received cetuximab and 10.7 months in the group who did not receive cetuximab (P = .01).
◦ In a subset analysis, cetuximab-treated patients with tumors bearing a mutated KRAS gene had significantly decreased PFS compared with cetuximab-treated patients with wild-type KRAS tumors (8.1 months vs. 10.5 months; P = .04).
◦ Cetuximab-treated patients with mutated KRAS tumors had a significantly shorter PFS compared with patients with mutated KRAS tumors who did not receive cetuximab (8.1 months vs. 12.5 months; P = .003) and a significantly shorter OS (17.2 months vs. 24.9 months; P = .03).
4. The Medical Research Council (MRC) (COIN [NCT00182715] trial) sought to answer the question of whether adding cetuximab to combination chemotherapy with a fluoropyrimidine and oxaliplatin in first-line treatment for patients with first-line KRAS wild-type tumors was beneficial.
◦ In addition, the MRC sought to evaluate the effect of intermittent chemotherapy versus continuous chemotherapy. The 1,630 patients were randomly assigned to three treatment groups:
• Arm A: fluoropyrimidine/oxaliplatin.
• Arm B: fluoropyrimidine/oxaliplatin/cetuximab.
• Arm C: intermittent fluoropyrimidine/oxaliplatin.
◦ The comparisons between arms A and B and arms A and C were analyzed and published separately.
◦ In patients with KRAS wild-type tumors (arm A, n = 367; arm B, n = 362), OS did not differ between treatment groups (median survival, 17.9 months [interquartile range (IQR) 10.3–29.2] in the control group vs. 17.0 months [IQR, 9.4–30.1] in the cetuximab group; HR, 1.04; 95% CI, 0.87–1.23; P = .67). Similarly, there was no effect on PFS (8.6 months [IQR, 5.0–12.5] in the control group versus 8.6 months [IQR, 5.1–13.8] in the cetuximab group; HR, 0.96; 95% CI, 0.82–1.12; P = .60).[Level of evidence: 1iiA]
◦ The reasons for lack of benefit in adding cetuximab are unclear. Subset analyses suggest that the use of capecitabine was associated with an inferior outcome, and the use of second-line therapy was less frequent in patients treated with cetuximab.
◦ There was no difference between the continuously treated patients (arm A) and the intermittently treated patients (arm C). Median survival in the intent-to-treat population (n = 815 in both groups) was 15.8 months (IQR, 9.4–26.1) in arm A and 14.4 months (IQR, 8.0–24.7) in arm C (HR, 1.084; 80% CI, 1.008–1.165). In the per-protocol population, which included only those patients who were free from progression at 12 weeks and randomly assigned to continue treatment or go on a chemotherapy holiday (arm A, n = 467; arm C, n = 511), median survival was 19.6 months (IQR, 13.0–28.1) in arm A and 18.0 months (IQR, 12.1–29.3) in arm C (HR, 1.087; 95% CI, 0.986–1.198). The upper limits of CIs for HRs in both analyses were greater than the predefined noninferiority boundary. While intermittent chemotherapy was not deemed noninferior, there appeared to be clinically insignificant differences in patient outcomes.
5.The OPUS study sought to evaluate the effect of adding cetuximab to first-line treatment with a FOLFOX regimen in an open-labeled, randomized, multicenter, phase II study of patients with EGFR-expressing metastatic colorectal cancer.
◦ In the trial, 344 patients were randomly assigned to receive FOLFOX-4 alone or FOLFOX-4/cetuximab. There was no statistically significant difference in response rate or PFS.
◦ On subset analysis, patients with KRAS wild-type tumors were analyzed separately. In the KRAS wild-type tumor population, there was a statistically significant improvement in response rate (61% vs. 37%, P = .011) and PFS (7.7 months vs. 7.2 months, P = .0163).
◦ On subset analysis, patients with KRAS mutant tumors receiving FOLFOX-4/cetuximab had a statistically significant worse PFS than patients with KRAS mutant tumors receiving FOLFOX-4 (5.5 months vs. 8.6 months, P = .0192).][Level of evidence: 1iiD]
■ Aflibercept
Aflibercept is a novel anti-VEGF molecule and has been evaluated as a component of second-line therapy in patients with metastatic colorectal cancer.
Evidence (afilbercept):
1. In one trial, 1,226 patients were randomly assigned to receive aflibercept (4 mg/kg IV) or placebo every 2 weeks in combination with FOLFIRI.[Level of evidence: 1A]
◦ Patients who received aflibercept/FOLFIRI had significantly improved OS rates, with median survival times of 13.50 months compared with patients who received placebo/FOLFIRI, with median survival times of 12.06 months (HR, 0.817; 95.34% CI, 0.713–0.937; P = .0032).
◦ Patients who received aflibercept/FOLFIRI also had significantly improved PFS rates, with median PFS rates of 6.90 months compared with patients who received placebo/FOLFIRI, with median PFS rates of 4.67 months (HR, 0.758; 95% CI, 0.661–0.869; P < .0001).
◦ On the basis of these results, the use of FOLFIRI/aflibercept is an acceptable second-line regimen for patients previously treated with FOLFOX-based chemotherapy. Whether to continue bevacizumab or initiate aflibercept in second-line therapy has not been addressed as yet in any clinical trial, and there are no data available.
■ Ramucirumab
Ramucirumab is a fully humanized monoclonal antibody that binds to vascular endothelial growth factor receptor-2.
Evidence (ramucirumab):
1. In the randomized, unblinded, phase III RAISE (NCT01183780) study, 1,072 patients with stage IV colorectal cancer who had progressed on first-line chemotherapy were randomly assigned to FOLFIRI with or without ramucirumab (8 mg/kg).[Level of evidence: 1iiA]
◦ Patients assigned to FOLFIRI/ramucirumab had a significant improvement in median OS (13.3 months vs. 11.7 months; HR, 0.84; P = .0219) and PFS (5.7 months vs. 4.5 months; HR, 0.793; P = .0005).
◦ Grade 3 adverse events were more common in the ramucirumab group, including grade 3 neutropenia.
◦ On the basis of this data, FOLFIRI/ramucirumab is an acceptable second-line regimen for patients previously treated with FOLFOX/bevacizumab. Whether to continue bevacizumab in second-line chemotherapy or use ramucirumab in second-line chemotherapy has not yet been addressed in a clinical trial.
■ Panitumumab
Panitumumab is a fully humanized antibody against the EGFR. The FDA approved panitumumab for use in patients with metastatic colorectal cancer refractory to chemotherapy. In clinical trials, panitumumab demonstrated efficacy as a single agent or in combination therapy, which was consistent with the effects on PFS and OS with cetuximab. There appears to be a consistent class effect.
Evidence (panitumumab):
1. In a phase III trial, patients with chemotherapy-refractory colorectal cancer were randomly assigned to panitumumab or best supportive care.[Level of evidence: 1iiDiii]
◦ Patients who received panitumumab experienced an improved PFS (8 weeks vs. 7.3 weeks; HR, 0.54; 95% CI, 0.44–0.66; P < .0001).
◦ There was no difference in OS, which was thought to be the result of 76% of patients on best supportive care crossing over to panitumumab.
2. In the Panitumumab Randomized Trial in Combination With Chemotherapy for Metastatic Colorectal Cancer to Determine Efficacy (PRIME) [NCT00364013] study, 1,183 patients were randomly assigned to FOLFOX-4 with or without panitumumab as first-line therapy for metastatic colorectal cancer. The study was amended to enlarge the sample size to address patients with the KRAS wild-type tumors and patients with mutant KRAS tumors separately.[Level of evidence: 1iiDiii]
1. For patients with KRAS wild-type tumors, a statistically significant improvement in PFS was observed in those who received panitumumab/FOLFOX-4 compared with those who received only FOLFOX-4 (HR, 0.80; 95% CI, 0.66–0.97; P = .02, stratified log-rank test).
2 .Median PFS was 9.6 months (95% CI, 9.2 months–11.1 months) for patients who received panitumumab/FOLFOX-4 and 8.0 months (95% CI, 7.5 months–9.3 months) for patients who received FOLFOX-4. OS was not significantly different between the groups (HR, 0.83; 95% CI, 0.67–1.02; P = .072).
3. For patients with mutant KRAS tumors, there was worse PFS with the addition of panitumumab (HR, 1.29; 95% CI, 1.04–1.62; P = .02, stratified log-rank test).
• Median PFS was 7.3 months (95% CI, 6.3 months–8.0 months) for panitumumab/FOLFOX-4 and 8.8 months (95% CI, 7.7 months–9.4 months) for FOLFOX-4 alone.
4.Subsequently, a retrospective analysis evaluated patients with wild-type KRAS exon 2 status for other KRAS and BRAF mutations.[Level of evidence: 3iiiA]
• Of the 620 patients who were initially identified as not having a mutation in exon 2 of KRAS, 108 patients (17%) were found to have additional RAS mutations and 53 patients (8%) were found to have BRAF mutations. In a retrospective analysis, patients without any RAS or BRAF mutations had a longer PFS (10.8 months vs. 9.2 months, P = .002) and OS (28.3 months vs. 20.9 months, P = .02) when assigned to the FOLFOX-4/panitumumab arm than the patients assigned to the FOLFOX-4 arm.
3. Similarly, the addition of panitumumab to a regimen of FOLFOX/bevacizumab resulted in a worse PFS and worse toxicity compared with a regimen of FOLFOX/bevacizumab alone in patients not selected for KRAS mutation in metastatic colon cancer (11.4 months vs. 10.0 months, HR, 1.27; 95% CI, 1.06–1.52).[Level of evidence: 1iiDiii]
4. In another study (NCT00339183), patients with metastatic colorectal cancer who had already received a fluoropyrimidine regimen were randomly assigned to either FOLFIRI or FOLFIRI/panitumumab.[Level of evidence: 1iiDiii]
1. In a post hoc analysis, patients with KRAS wild-type tumors experienced a statistically significant PFS advantage (HR, 0.73; 95% CI, 0.59–0.90; P = .004, stratified log-rank).
• Median PFS was 5.9 months (95% CI, 5.5 months–6.7 months) for panitumumab/FOLFIRI and 3.9 months (95% CI, 3.7 months–5.3 months) for FOLFIRI alone.
2. OS was not significantly different. Patients with mutant KRAS tumors experienced no benefit from the addition of panitumumab.
Anti-EGFR antibody versus anti-VEGF antibody with first-line chemotherapy
In the management of patients with stage IV colorectal cancer, it is unknown whether patients with KRAS wild-type cancer should receive an anti-EGFR antibody with chemotherapy or an anti-VEGF antibody with chemotherapy. Two studies attempted to answer this question.
Evidence (anti-EGFR antibody vs. anti-VEGF antibody with first-line chemotherapy)
1. The FIRE-3 [NCT00433927] study randomly assigned 592 patients with KRAS exon 2 wild-type tumors who were previously untreated to FOLFIRI/cetuximab (297 patients) or FOLFIRI/bevacizumab (295 patients). The primary endpoint of the study was objective response rate.[[Level of evidence: 1iiA]
◦ The objective response rate was not significantly different between the groups (objective response rate, 62.0%; 95% CI, 56.2–67.5 vs. objective response rate, 58.0%; 95% CI, 52.1–63.7; OR, 1.18; 95% CI, 0.85–1.64; P = .18).
◦ Median PFS was 10.0 months (95% CI, 8.8–10.8) in the cetuximab group and 10.3 months (95% CI, 9.8–11.3) in the bevacizumab group (HR, 1.06; 95% CI, 0.88–1.26; P = .55).
◦ Median OS was 28.7 months (95% CI, 24.0–36.6) in the cetuximab group compared with 25.0 months (22.7–27.6) in the bevacizumab group (HR, 0.77; 95% CI, 0.62–0.96; P = .017).
◦ In a post hoc analysis of patients with expanded RAS wild-type tumors (sequencing for mutational hot spots within KRAS and NRAS genes, including exon 2 codons 12 and 13; exon 3 codons 59 and 61; and exon 4 codons 117 and 146), the median OS was 33.1 months (95% CI, 24.5–39.4) in the cetuximab group compared with 25.0 months (95% CI, 23.0–28.1) in the bevacizumab group (HR, 0.70; 95% CI, 0.54–0.90; P = .0059).
◦ Of note, only 52% of patients assigned to the bevacizumab arm subsequently received cetuximab or panitumumab.
2. The Cancer and Leukemia Group B Intergroup study 80405 [NCT00265850] was presented at the ASCO meeting in 2014. This study randomly assigned 2,334 previously untreated patients with KRAS wild-type cancer to chemotherapy (FOLFOX or FOLFIRI) plus bevacizumab or chemotherapy/cetuximab. OS was the primary endpoint.[Level of evidence: 1iiDiii]
◦ There was no statistically significant difference in OS among the patients assigned to bevacizumab or cetuximab (for OS differences, chemotherapy/bevacizumab = 29.04 [25.66–31.21] months vs. chemotherapy/cetuximab = 29.93 [27.56–31.21] months; HR, 0.92 [0.78, 1.09]; P = .34).
On the basis of these two studies, no apparent significant difference is evident about starting treatment with chemotherapy/bevacizumab or chemotherapy/cetuximab in patients with KRAS wild-type metastatic colorectal cancer. However, in patients with KRAS wild-type cancer, administration of an anti-EGFR antibody at some point in the course of management improves OS.
■ Regorafenib
Regorafenib is an inhibitor of multiple tyrosine kinase pathways including VEGF. In September 2012, the FDA granted approval for the use of regorafenib in patients who had progressed on previous therapy.
Evidence (regorafenib):
1. The safety and effectiveness of regorafenib were evaluated in a single, clinical study of 760 patients with previously treated metastatic colorectal cancer. Patients were randomly assigned in a 2:1 fashion to receive regorafenib or a placebo in addition to the best supportive care.
◦ Patients treated with regorafenib had a statistically significant improvement in OS (6.4 months in the regorafenib group vs. 5.0 months in the placebo group; HR, 0.77; 95% CI, 0.64–0.94; one-sided P = .0052).
■ TAS-102
TAS-102 (Lonsurf) is an orally administered combination of a thymidine-based nucleic acid analog, trifluridine, and a thymidine phosphorylase inhibitor, tipiracil hydrochloride. Trifluridine, in its triphosphate form, inhibits thymidylate synthase; therefore, trifluridine, in this form, has an anti-tumor effect. Tipiracil hydrochloride is a potent inhibitor of thymidine phosphorylase, which actively degrades trifluridine. The combination of trifluridine and tipiracil allows for adequate plasma levels of trifluridine.
Evidence (TAS-102):
1. A phase III, double-blind study (RECOURSE [NCT01607957]) randomly assigned 800 stage IV colorectal cancer patients whose cancer had been refractory to two previous therapies. Patients were required to have received 5-FU, oxaliplatin, irinotecan, bevacizumab and, if the patients had KRAS wild-type cancer, cetuximab or panitumumab. Patients were randomly assigned in a 2:1 ratio to receive best supportive care plus TAS-102 (n = 534) or placebo (n = 266). The median age of patients was 63 years, and the majority of patients (60%–63%) received four or more previous lines of therapy. All patients had formerly received fluoropyrimidine, irinotecan, oxaliplatin, and bevacizumab, and 52% of them had received an EGFR inhibitor. Approximately 20% of the patients had received previous treatment with regorafenib.[Level of evidence: 1iiA]
◦ TAS-102 was administered at 35 mg/m2 twice daily with meals for 5 days, with 2 days of rest for 2 weeks, followed by a 14-day rest period.
◦ The primary endpoint of the study was OS. The median OS for patients with metastatic colorectal cancer who received TAS-102 was 7.1 months compared with 5.3 months for those who received a placebo (HR, 0.68; P < .0001).
◦ The median PFS time in the TAS-102 arm was 2 months versus 1.7 months with a placebo (HR, 0.48; P < .0001).
◦ Secondary endpoints focused on PFS, overall response rate, and disease control rate.
◦ The overall response rate was 1.6% with TAS-102, which consisted of a complete response in one patient and partial responses in other patients. The overall response rate with a placebo was 0.4% (P = .29).
TAS-102 was approved by the FDA for the treatment of metastatic colorectal cancer patients, based on the results of the RECOURSE trial.
Treatment Options Under Clinical Evaluation
1. Clinical trials evaluating new drugs and biological therapy.
2. Clinical trials comparing various chemotherapy regimens or biological therapy, alone or in combination.
Colon Cancer - Treatment Options
Colorectal Cancer - Treatment Options
(Updated 08/2017)
Treatment overview
In cancer care, different types of doctors often work together to create a patient’s overall treatment plan that usually includes or combines different types of treatments. This is called a multidisciplinary team. For colorectal cancer, this generally includes a surgeon, medical oncologist, radiation oncologist, and a gastroenterologist. Cancer care teams include a variety of other health care professionals, such as physician assistants, oncology nurses, social workers, pharmacists, counselors, dietitians, and others.
Descriptions of the most common treatment options for colorectal cancer are listed below, followed by a brief outline of treatment options listed by stage. Treatment options and recommendations depend on several factors, including the type and stage of cancer, possible side effects, and the patient’s preferences and overall health. Your care plan may also include treatment for symptoms and side effects, an important part of cancer care.
Studies have shown that these various treatment approaches provide similar benefits regardless of the patient’s age. However, older patients may have unique treatment challenges. In order to tailor the treatment to each patient, all treatment decisions should consider such factors as:
• The patient’s other medical conditions
• The patient’s overall health
• Potential side effects of the treatment plan
• Other medications that the patient already takes
• The patient’s nutritional status and social support
(More information on the specific effects of surgery, chemotherapy, and radiation therapy on older patients can be found in this article in another section of Cancer.Net. )
Surgery
Surgery is the removal of the tumor and some surrounding healthy tissue during an operation. This is the most common treatment for colorectal cancer and is often called surgical resection. Part of the healthy colon or rectum and nearby lymph nodes will also be removed.
In addition to surgical resection, surgical options for colorectal cancer include:
• Laparoscopic surgery. Some patients may be able to have laparoscopic colorectal cancer surgery. With this technique, several viewing scopes are passed into the abdomen while a patient is under anesthesia. Anesthesia is medicine that blocks the awareness of pain. The incisions are smaller and the recovery time is often shorter than with standard colon surgery. Laparoscopic surgery is as effective as conventional colon surgery in removing the cancer. Surgeons who perform laparoscopic surgery have been specially trained in that technique.
• Colostomy for rectal cancer. Less often, a person with rectal cancer may need to have a colostomy. This is a surgical opening, or stoma, through which the colon is connected to the abdominal surface to provide a pathway for waste to exit the body. This waste is collected in a pouch worn by the patient. Sometimes, the colostomy is only temporary to allow the rectum to heal, but it may be permanent. With modern surgical techniques and the use of radiation therapy and chemotherapy before surgery when needed, most people who receive treatment for rectal cancer do not need a permanent colostomy. Learn more about colostomies.
• Radiofrequency ablation (RFA) or cryoablation. Some patients may be able to have surgery on the liver or lungs to remove tumors that have spread to those organs. Other ways include using energy in the form of radiofrequency waves to heat the tumors, called RFA, or to freeze the tumor, called cryoablation. Not all liver or lung tumors can be treated with one of these approaches. RFA can be done through the skin or during surgery. While this can help avoid removing parts of the liver and lung tissue that might be removed in a regular surgery, there is also a chance that parts of tumor will be left behind.
Side effects of surgery
In general, the side effects of surgery include pain and tenderness in the area of the operation. The operation may also cause constipation or diarrhea, which usually goes away after a while. People who have a colostomy may have irritation around the stoma. If you need to have a colostomy, the doctor, nurse, or an enterostomal therapist, who is a specialist in colostomy management, can teach you how to clean the area and prevent infection.
Many people need to retrain their bowel after surgery, which may take some time and assistance. You should talk with your doctor if you do not regain good control of bowel function.
Radiation therapy
Radiation therapy is the use of high-energy x-rays to destroy cancer cells. It is commonly used for treating rectal cancer because this tumor tends to recur near where it originally started.
• External-beam radiation therapy. External-beam radiation therapy uses a machine to deliver x-rays to where the cancer is located. Radiation treatment is usually given 5 days a week for several weeks. It may be given in the doctor's office or at the hospital.
• Stereotactic radiation therapy. Stereotactic radiation therapy is a type of external-bean radiation therapy that may be used if a tumor has spread to the liver or lungs. This type of radiation therapy delivers a large, precise radiation dose to a small area. This technique can help avoid removing parts of the liver and lung tissue that might be removed during surgery. However, not all cancers that have spread to the liver or lungs can be treated in this way.
• Other types of radiation therapy. For some people, specialized radiation therapy techniques, such as intraoperative radiation therapy or brachytherapy, may help get rid of small areas of cancer that could not be removed with surgery.
• Intraoperative radiation therapy. Intraoperative radiation therapy uses a high, single dose of radiation therapy given during surgery.
• Brachytherapy. Brachytherapy is the use of radioactive "seeds" placed inside the body. In 1 type of brachytherapy with a product called SIR-Spheres, tiny amounts of a radioactive substance called yttrium-90 are injected into the liver to treat colorectal cancer that has spread to the liver when surgery is not an option. While limited information is available about how effective this approach is, some studies suggest that it may help slow the growth of cancer cells.
• Radiation therapy for rectal cancer. For rectal cancer, radiation therapy may be used before surgery, called neoadjuvant therapy, to shrink the tumor so that it is easier to remove. It may also be used after surgery to destroy any remaining cancer cells. Both approaches have worked to treat this disease. Chemotherapy is often given at the same time as radiation therapy, called chemoradiation therapy, to increase the effectiveness of the radiation therapy. Chemoradiation therapy is often used in rectal cancer before surgery to avoid colostomy or reduce the chance that the cancer will recur. One study found that chemoradiation therapy before surgery worked better and caused fewer side effects than the same radiation therapy and chemotherapy given after surgery. The main benefits included a lower rate of the cancer coming back in the area where it started, fewer patients who needed permanent colostomies, and fewer problems with scarring of the bowel where the radiation therapy was given.
Side effects of radiation therapy
Side effects from radiation therapy may include fatigue, mild skin reactions, upset stomach, and loose bowel movements. It may also cause bloody stools from bleeding through the rectum or blockage of the bowel. Most side effects go away soon after treatment is finished.
Sexual problems, as well as infertility (the inability to have a child) in both men and women, may occur after radiation therapy to the pelvis. Before treatment begins, talk with your doctor about the possible sexual and fertility-related side effects of your treatment and the available options for preserving fertility.
Chemotherapy
Chemotherapy is the use of drugs to destroy cancer cells, usually by ending the cancer cells’ ability to grow and divide.
Chemotherapy may be given after surgery to eliminate any remaining cancer cells. For some people with rectal cancer, the doctor will give chemotherapy and radiation therapy before surgery to reduce the size of a rectal tumor and reduce the chance of the cancer returning.
Types of chemotherapy for colorectal cancer
Currently, several drugs are approved by the U.S. Food and Drug Administration (FDA) to treat colorectal cancer in the United States. Your doctor may recommend 1 or more of them at different times during treatment. Sometimes these are combined with targeted therapy drugs (see “Targeted therapy” below).
• Capecitabine (Xeloda)
• Fluorouracil (5-FU, Adrucil)
• Irinotecan (Camptosar)
• Oxaliplatin (Eloxatin)
• Trifluridine/tipiracil (TAS-102, Lonsurf)
Some common treatment regimens using these drugs include:
• 5-FU
• 5-FU with leucovorin (Wellcovorin), a vitamin that improves the effectiveness of 5-FU
• Capecitabine, an oral form of 5-FU
• FOLFOX: 5-FU with leucovorin and oxaliplatin
• FOLFIRI: 5-FU with leucovorin and irinotecan
• Irinotecan alone
• XELIRI/CAPIRI: Capecitabine with irinotecan
• XELOX/CAPEOX: Capecitabine with oxaliplatin
• Any of the above with 1 of the following targeted therapies (see below): cetuximab, bevacizumab, or panitumumab. In addition, FOLFIRI may be combined with either of these targeted therapies (see below): ziv-aflibercept or ramucirumab
Side effects of chemotherapy
Chemotherapy may cause vomiting, nausea, diarrhea, neuropathy, or mouth sores. However, medications to prevent these side effects are available. Because of the way drugs are given, these side effects are less severe than they have been in the past for most patients. In addition, patients may be unusually tired, and there is an increased risk of infection. Neuropathy, tingling or numbness in feet or hands, may also occur with some drugs. Significant hair loss is an uncommon side effect with many of the drugs used to treat colorectal cancer, except irinotecan.
If side effects are particularly difficult, the dose of the drug may be lowered or a treatment session may be postponed. If you are receiving chemotherapy, you should talk with your health care team about when to call your doctor about side effects. Read more about managing side effects. The side effects from chemotherapy usually go away after treatment is finished.
Targeted therapy
(Updated 10/2017)
Targeted therapy is a treatment that targets the cancer’s specific genes, proteins, or the tissue environment that contributes to cancer growth and survival. This type of treatment blocks the growth and spread of cancer cells while limiting damage to healthy cells.
Recent studies show that not all tumors have the same targets. To find the most effective treatment, your doctor may run tests to identify the genes, proteins, and other factors in your tumor. This helps doctors better match each patient with the most effective treatment whenever possible. In addition, many research studies are taking place now to find out more about specific molecular targets and new treatments directed at them. These drugs are becoming more important in the treatment of colorectal cancer.
Studies have shown that older patients are able to benefit from targeted therapies, similar to younger patients. In addition, the expected side effects are usually manageable in both older and younger patients.
Types of targeted therapy
For colorectal cancer, the following targeted therapies may be options.
• Anti-angiogenesis therapy. Anti-angiogenesis therapy is a type of targeted therapy. It is focused on stopping angiogenesis, which is the process of making new blood vessels. Because a tumor needs the nutrients delivered by blood vessels to grow and spread, the goal of anti-angiogenesis therapies is to “starve” the tumor.
• Bevacizumab (Avastin). When bevacizumab is given with chemotherapy, it increases the length of time patients with advanced colorectal cancer live. In 2004, the FDA approved bevacizumab along with chemotherapy as the first treatment, or first-line treatment, for advanced colorectal cancer. Recent studies have shown it is also effective as second-line therapy along with chemotherapy. A similar drug called bevacizumab-awwb (Mvasi) received FDA approval in 2017.
• Regorafenib (Stivarga). This drug was approved in 2012 for patients with metastatic colorectal cancer who have already received certain types of chemotherapy and other targeted therapies.
• Ziv-aflibercept (Zaltrap) and ramucirumab (Cyramza). Either of these drugs can be combined with FOLFIRI chemotherapy as a second-line treatment for metastatic colorectal cancer.
• Epidermal growth factor receptor (EGFR) inhibitors. An EGFR inhibitor is a type of targeted therapy. Researchers have found that drugs that block EGFR may be effective for stopping or slowing the growth of colorectal cancer.
• Cetuximab (Erbitux). Cetuximab is an antibody made from mouse cells that still has some of the mouse structure.
• Panitumumab (Vectibix). Panitumumab is made entirely from human proteins and is less likely to cause an allergic reaction than cetuximab.
Recent studies show that cetuximab and panitumumab do not work as well for tumors that have specific mutations, or changes, to a gene called RAS. ASCO recommends that all patients with metastatic colorectal cancer who may receive anti-EFGR therapy, such as cetuximab and panitumumab, have their tumors tested for RAS gene mutations. If a patient’s tumor has a mutated form of the RAS gene, ASCO recommends against the use of EFGR inhibitors. Furthermore, the FDA now recommends that both cetuximab and panitumumab only be given to patients with a tumor with non-mutated, sometimes called wild-type, RAS genes.
• Checkpoint inhibitors (immunotherapy). Immunotherapy is a way to boost the body's natural defenses to fight the cancer.
•Pembrolizumab (Keytruda). Pembrolizumab is a humanized antibody that targets PD-1, a receptor on tumor cells, preventing the tumor cells from hiding from the immune system. A humanized antibody combines a human antibody with a small part of a mouse or rat antibody. The mouse or rat part binds to the target, and the human part makes it less likely to be destroyed by the body's immune system. Pembrolizumab is FDA approved for treating metastatic colorectal cancers that have a molecular feature called microsatellite instability (MSI-H) or mismatch repair deficiency (dMMR).
•Nivolumab (Opdivo). Nivolumab is a checkpoint inhibitor that has received FDA approval to treat patients who are 12 or older and have MSI-H or dMMR metastatic colorectal cancer that has grown or spread after treatment with chemotherapy with a fluoropyrimidine (such as capecitabine and fluorouracil), oxaliplatin, and irinotecan.
Your tumor may also be tested for other molecular markers, including BRAF, HER2 overexpression, and others. These markers do not have FDA-approved targeted therapies yet, but there may be opportunities in clinical trials that are studying these molecular changes.
Side effects of targeted therapies
The side effects of targeted treatments can include a rash to the face and upper body, which can be prevented or reduced with various treatments. Find out more about skin reactions to targeted therapies.
Getting care for symptoms and side effects
Cancer and its treatment often cause side effects. In addition to treatments intended to slow, stop, or eliminate the cancer, an important part of cancer care is relieving a person’s symptoms and side effects. This approach is called palliative or supportive care, and it includes supporting the patient with his or her physical, emotional, and social needs.
Palliative care is any treatment that focuses on reducing symptoms, improving quality of life, and supporting patients and their families. Any person, regardless of age or type and stage of cancer, may receive palliative care. It works best when palliative care is started as early as needed in the cancer treatment process. People often receive treatment for the cancer at the same time that they receive treatment to ease side effects. In fact, patients who receive both at the same time often have less severe symptoms, better quality of life, and report they are more satisfied with treatment.
Palliative treatments vary widely and often include medication, nutritional changes, relaxation techniques, emotional support, and other therapies. You may also receive palliative treatments similar to those meant to eliminate the cancer, such as chemotherapy, surgery, or radiation therapy. Talk with your doctor about the goals of each treatment in the treatment plan.
Before treatment begins, talk with your health care team about the possible side effects of your specific treatment plan and palliative care options. During and after treatment, be sure to tell your doctor or another health care team member if you are experiencing a problem so it can be addressed as quickly as possible. Learn more about palliative care.
Treatment options by stage
In general, stages 0, I, II, and III are often curable with surgery. However, many patients with stage III colorectal cancer, and some with stage II, receive chemotherapy after surgery to increase the chance of eliminating the disease. Patients with stage II and III rectal cancer will also receive radiation therapy with chemotherapy either before or after surgery. Stage IV is not often curable, but it is treatable, and the growth of the cancer and the symptoms of the disease can be managed. Clinical trials are also a treatment option for each stage.
Stage 0 colorectal cancer
The usual treatment is a polypectomy, or removal of a polyp, during a colonoscopy. There is no additional surgery unless the polyp cannot be fully removed.
Stage I colorectal cancer
Surgical removal of the tumor and lymph nodes is usually the only treatment needed.
Stage II colorectal cancer
Surgery is often the first treatment. Patients with stage II colorectal cancer should talk with their doctor about whether more treatment is needed after surgery because some patients receive adjuvant chemotherapy. Adjuvant chemotherapy is treatment after surgery aimed at trying to destroy any remaining cancer cells. However, cure rates for surgery alone are quite good, and there are few benefits of additional treatment for people with this stage of colorectal cancer. Learn more about adjuvant therapy for stage II colorectal cancer. A clinical trial is also an option after surgery.
For patients with stage II rectal cancer, radiation therapy is usually given in combination with chemotherapy, either before or after surgery. Additional chemotherapy may be given after surgery as well.
Stage III colorectal cancer
Treatment usually involves surgical removal of the tumor fo llowed by adjuvant chemotherapy. A clinical trial may also an option. For patients with rectal cancer, radiation therapy may be used along with chemotherapy before or after surgery, along with adjuvant chemotherapy.
Metastatic (stage IV) colorectal cancer
If cancer spreads to another part in the body from where it started, doctors call it metastatic cancer. Colorectal cancer can spread to distant organs, such as the liver, lungs, the tissue called the peritoneum that lines the abdomen, or a woman’s ovaries. If this happens, it is a good idea to talk with doctors who have experience treating this stage of cancer. Doctors can have different opinions about the best standard treatment plan. Also, clinical trials might be an option.
Your treatment plan may include a combination of surgery, radiation therapy, immunotherapy, and chemotherapy, which can be used to slow the spread of the disease and often temporarily shrink a cancerous tumor. Palliative care will also be important to help relieve symptoms and side effects.
At this stage, surgery to remove the portion of the colon where the cancer started usually cannot cure the cancer, but it can help relieve blockage of the colon or other problems related to the cancer. Surgery may also be used to remove parts of other organs that contain cancer, called resection, and can cure some people if a limited amount of cancer spreads to a single organ, such as the liver or a lung.
In colorectal cancer, if the cancer has spread only to the liver and if surgery is possible—either before or after chemotherapy—there is a chance of complete cure. Even when curing the cancer is not possible, surgery may add months or even years to a person’s life. Determining who can benefit from surgery for cancer that has spread to the liver is often a complicated process that involves doctors of multiple specialties working together to plan the best treatment option.
For most patients, a diagnosis of metastatic cancer is very stressful and, at times, difficult to bear. Patients and their families are encouraged to talk about the way they are feeling with doctors, nurses, social workers, or other members of the health care team. It may also be helpful to talk with other patients, including through a support group.
Systemic Treatments
Neoadjuvant therapy for resectable metastatic disease
Neoadjuvant therapy for resectable metastatic disease is usually administered for approximately 2-3 months, limiting the development of hepatotoxicity.
Regimens for adjuvant and neoadjuvant therapy are similar:
• mFOLFOX6
• FOLFIRI:
Irinotecan 180 mg/m2 IV over 30-90 min on day 1 plus
leucovorin 400 mg/m2 IV infusion to match duration of irinotecan infusion on day 1 plus
5-FU 400 mg/m2 IV bolus on day 1, then 1200 mg/m2/day for 2 days (total 2400 mg/m2 over 46-48 hours) continuous infusion;
Repeat every 2 wk
• CapeOx with or without bevacizumab:
Oxaliplatin 130 mg/m2 over 2 h on day 1
capecitabine 1000 mg/m2 PO BID for 14 d;
bevacizumab 7.5 mg/kg IV on day 1
Repeat every 3 wk
• mFOLFOX6 plus bevacizumab: Bevacizumab 5 mg/kg over 30-90 min on day 1
Repeat every 2 wk for four to six cycles with reevaluation for maintenance therapy
• FOLFIRI plus bevacizumab: Bevacizumab 5 mg/kg over 30-90 min on day 1
Repeat every 2 wk for 4-6 cycles
• mFOLFOX6 plus cetuximab (only for pan-RAS wild-type tumors): Cetuximab 400 mg/m2 loading dose over 2 h on day 1, then cetuximab 250 mg/m2 weekly
Repeat every 2 wk for 4-6 cycles
• FOLFIRI plus cetuximab (only for pan-RAS wild-type tumors): Cetuximab 400 mg/m2 loading dose over 2 hours on day 1, then cetuximab 250 mg/m2 over 1 hour weekly
Repeat every 2 wk for 4-6 cycles
• FOLFOXIRI:
Irinotecan 165 mg/m 2 over 60 minutes then
oxaliplatin 85 mg/m 2 plus
leucovorin 400 mg/m 2 concurrently over 120 minutes then
5-FU 1600 mg/m 2/day for 2 days (total 3200 mg/m 2 over 48 hours);
Repeat every 2 wk for 4-6 cycles
• FOLFOXIRI plus bevacizumab: Bevacizumab 5 mg/kg IV over 30-90 min plus FOLFOXIRI
Repeat every 2 wk for 4-6 cycles
Summary of guiding principles in the treatment of metastatic colorectal cancer
• Differentiating M1a (metastatic disease at one organ site) from M1b (metastasis at more than one organ site) is important, in view of the curative potential of M1a disease.
• It is reasonable to leave the primary therapy in place when starting treatment for metastatic disease, if the patient has no urgent complication such as obstruction or uncontrolled bleeding.
• A multidisciplinary approach is necessary to deal with the complicated issue of potentially resectable or marginally resectable metastatic disease.
• Patients who receive bevacizumab-containing neoadjuvant therapy must not undergo surgery until at least 6-8 weeks afterward, in order to minimize perioperative complications.
• With FOLFOXIRI, a lower dose of infusional 5-FU at 2400 mg/m2 should be considered in North American patients. This regimen has the advantage of increased response rate, R0 resection margin of metastatic disease, progression-free survival, and overall survival compared with FOLFIRI and should be used selectively in patients with good performance status, particularly when the goal is to render the patient cancer free with neoadjuvant therapy. The same is true if bevacizumab is to be added.
• The selection of oxaliplatin or irinotecan as part of the cytotoxic backbone upfront in metastatic disease is based primarily on toxicity profile.
• Bevacizumab, when used as first-line and second-line therapy and works with irinotecan- and oxaliplatin-based therapy, improves survival.
• Bevacizumab, when added to fluorouracil-based combination chemotherapy, results in statistically significant and clinically meaningful improvement in survival among patients with metastatic colorectal cancer.
• Bevacizumab, when added to IFL (irinotecan, fluorouracil, and leucovorin), significantly improves the response rate, overall survival, and progression-free survival.
• Interruption in therapy is not ideal for patients; some form of maintenance therapy is preferred after a stable disease state is obtained.
• Single-agent maintenance bevacizumab may be a feasible option for patients receiving bevacizumab + CapeOx as induction therapy.
• Anti-EGFR antibody therapy should be given only to patients with pan-RAS and BRAF V600E wild-type tumors.
• Anti-EGFR antibody therapy and bevacizumab should not be combined, due to increased toxicity.
• All patients with metastatic disease should have pan-RAS testing and BRAF V600E mutation testing. Data suggest that even in the setting of KRAS wild-type tumors, BRAF mutation abrogates the effect of anti-EGFR antibody therapy; it is, however, prognostic of a worse outcome.
• Patients with stage IV disease should be tested for MSI-H.
Consider pembrolizumab or nivolumab for unresectable or metastatic colon cancer that has tested positive for MSI-H or dMMR, and has progressed following treatment with a fluoropyrimidine (eg, 5-FU, capecitabine), oxaliplatin, and irinotecan.
Chemotherapy for advanced or metastatic disease
In patients with metastatic colon cancer, testing of the tumor for KRAS mutations at exons 2, 3, and 4; NRAS mutations at exons 2, 3, and 4 (ie, pan-RAS or all-RAS testing) and BRAF V600E mutation should guide the decision whether to use biologic agents that target epidermal growth factor receptor (EGFR). Patients with wild-type pan-RAS and no BRAF V600E typically respond to anti-EGFR therapy.
Stage IV:
Chemotherapy for advanced or metastatic disease includes the use of multiple drugs as single agents or as combination regimens, as follows:
• Patients with right sided tumors are less likely to respond to EGFR therapy with cetuximab or panitumumab.
• BRAF V600E mutation makes response to anti-EGFR therapy less likely.
• Choice of initial therapy for advanced disease is based on goals of treatment, location of tumor, mutational profile, toxicity profile of the drugs, and patient's performance status.
• mFOLFOX6, FOLFIRI, CapeOx, FOLFOXIRI, capecitabine, and infusional 5FU/LV with or without targeted agents are all considered appropriate first-line agents.
• For patients who are not candidates for intensive therapy, single-agent 5FU/LV, capecitabine, irinotecan, cetuximab or panitumumab, and nivolumab or pembrolizumab, can be used in the appropriate setting.
First-line chemotherapy for bevacizumab candidates:
mFOLFOX6 plus bevacizumab
FOLFIRI plus bevacizumab
FOLFOXIRI plus bevacizumab
CAPEOX plus bevacizumab
Capecitabine plus bevacizumab
DeGramont regimen plus bevacizumab (in patients not able to undergo treatment with oxaliplatin or irinotecan):
Bevacizumab 5 mg/kg over 30-90 min on day 1 plus
leucovorin 400 mg/m2 IV over 2 h on day 1 plus
5-FU bolus 400 mg/m2, then 1200 mg/m2/day for 2 days (total 2400 mg/m2 over 46-48 h) continuous infusion;
Repeat every 2 wk for 4-6 cycles with reevaluation for maintenance therapy
5-FU and leucovorin (Roswell Park) with bevacizumab (in patients unable to undergo treatment with oxaliplatin or irinotecan):
Bevacizumab 5 mg/kg over 30-90 min on day 1 plus
leucovorin 500 mg/m2 over 2 h plus
5-FU 500 mg/m2 bolus every 2 wk for 4-6 cycles with reevaluation for maintenance therapy
First-line chemotherapy for patients who are not candidates for bevacizumab:
mFOLFOX6
mFOLFOX7: Oxaliplatin 85 mg/m2 IV over 2 h on day 1 plus leucovorin 400 mg/m2 IV over 2 h on day 1 plus 5-FU 1200mg/m2/day (total 2400 mg/m2 over 46-48 hours) continuous infusion; repeat every 2 wk
FOLFIRI
FOLFOXIRI
Capecitabine: Capecitabine 850-1250 mg/m2 PO BID on days 1-14; repeat cycle every 21 d until progression
Roswell Park regimen: Leucovorin 500 mg/m2 IV weekly for 6 wk over 2 h followed by 5-FU 500 mg/m2 IV bolus weekly for 6 wk; repeat cycle every 8 wk
CapeOx
mFOLFOX6 plus cetuximab (only for pan-RAS and BRAF V600E wild-type tumors): Cetuximab 500 mg/mg/m2 IV over 2 h every 2 weeks or cetuximab 400 mg/m2 loading dose on day 1, then cetuximab 250 mg/m2 weekly plus oxaliplatin 85 mg/m2 IV over 2 h on day 1 plus leucovorin 400 mg/m2 IV over 2 h on day 1 plus 5-FU 400 mg/m2 IV bolus on day 1, then 1200 mg/m2/day for 2-d (total 2400 mg/m2 over 46 h) continuous infusion; repeat every 2 wk
FOLFIRI plus cetuximab (only for pan-RAS and BRAF V600E wild-type tumors): Cetuximab 500 mg/m2 IV over 2 hr every 2 weeks or cetuximab 400 mg/m2 loading dose over 2 h on day 1, then cetuximab 250 mg/m2 over 1 h weekly plus irinotecan 180 mg/m2 IV over 30-90 min on day 1 plus leucovorin 400 mg/m2 IV infusion to match duration of irinotecan infusion on day 1 plus 5-FU 400 mg/m2 IV bolus on day 1, then 1200 mg/m2/day for 2-d (total 2400 mg/m2 over 46 h) continuous infusion; repeat every 2 wk
FOLFOX plus panitumumab (only for pan-RAS and BRAF V600E wild-type tumors): Panitumumab 6 mg/kg IV infusion over 1 h on day 1, then oxaliplatin 85 mg/m2 IV infusion on day 1, then leucovorin 400 mg/m2 IV infusion, plus 5-FU 400 mg/m2 IV bolus on day 1, then 1200 mg/m2/day for 2 d (total 2400 mg/m2 over 46-48 h) continuous infusion; repeat every 2 wk
FOLFOX4 plus panitumumab (only for pan-RAS and BRAF V600E wild-type tumors): Panitumumab 6 mg/kg IV infusion over 1 h on day 1, then oxaliplatin 85 mg/m2 IV infusion on day 1 then leucovorin 200 mg/m2 (or equivalent) IV infusion plus 5-FU 400 mg/m2 IV bolus and 600 mg/m2 22-hour continuous infusion on days 1 and 2
FOLFIRI plus panitumumab (only for pan-RAS and BRAF V600E wild-type tumors): Panitumumab 6 mg/kg IV infusion over 1 h on day 1 plus irinotecan 180 mg/m2 IV over 30-90 min on day 1 plus leucovorin 400 mg/m2 IV infusion to match duration of irinotecan infusion on day 1 plus 5-FU 400 mg/m2 IV bolus on day 1, then 1200 mg/m2/day for 2-d (total 2400 mg/m2 over 46 h) continuous infusion; repeat every 2 wk
Referral for clinical trial
Second-line chemotherapy for metastatic disease:
Subsequent therapy primarily depends on the initial therapy—oxaliplatin vs irinotecan based, as follows:
Bevacizumab is indicated for second-line treatment in patients whose disease has progressed on a first-line bevacizumab-containing regimen; use bevacizumab in combination with a fluoropyrimidine (eg, 5-FU, capecitabine) plus irinotecan or oxaliplatin-based chemotherapy; bevacizumab dose is either 5 mg/kg IV q2 wk or 7.5 mg/kg IV q3 wk for continuation
Ziv-aflibercept and ramucirumab are effective only in combination with FOLFIRI, in patients that have not previously received treatment with FOLFIRI.
Cetuximab and panitumumab (anti-EGFR) can also be used as single agents for patients who cannot tolerate chemotherapy.
For patients with previous oxaliplatin-based therapy as first-line treatment (ie, FOLFOX, CapeOx, CapeOx plus bevacizumab or FOLFOX plus bevacizumab), one of the following regimens can be used:
FOLFIRI
FOLFIRI + Bevacizumab or ziv-aflibercept or ramucirumab: Irinotecan 180 mg/m2 IV over 30-90 min on day 1 plus leucovorin 400 mg/m2 IV infusion to match duration of irinotecan infusion on day 1 plus 5-FU 400 mg/m2 IV bolus on day 1, then 1200 mg/m2/day for 2-d (total 2400 mg/m2 over 46 h) continuous infusion plus bevacizumab 5mg/kg iv on day 1 or ziv-aflibercept 4mg/kg iv over 60 mins on day 1 or ramucirumab 8mg/kg iv over 60 mins on day 1, repeat every 2 wk
FOLFIRI plus cetuximab or panitumumab (only for pan-RAS and BRAF V600E wild-type tumors): Cetuximab 400 mg/m 2 loading dose IV over 2 h on day 1, then cetuximab 250 mg/m 2 IV over 1 h weekly or panitumumab 6 mg/kg IV over 60 mins on day 1 plus irinotecan 180 mg/m 2 IV over 30-90 min on day 1 plus leucovorin 400 mg/m 2 IV infusion to match duration of irinotecan infusion on day 1 plus 5-FU 400 mg/m 2 IV bolus on day 1, then 1200 mg/m 2/day for 2-d (total 2400 mg/m 2 over 46-48 h) continuous infusion; repeat every 2 wk for 4-6 cycles, then reevaluate
Irinotecan plus cetuximab or panitumumab (only for pan-RAS and BRAF V600E wild-type tumors): Irinotecan 180 mg/m2 IV over 30-90 min on day 1 plus cetuximab 400 mg/m2 loading dose over 2 h on day 1, then cetuximab 250 mg/m2 over 1 h weekly or panitumumab 6 mg/kg iv over 60 min on day 1; repeat every 2 wk
For patients who had irinotecan therapy as first-line treatment (ie, FOLFIRI plus bevacizumab), the following regimens can be used:
mFOLFOX6
CapeOx
FOLFOX plus bevacizumab
CapeOx plus bevacizumab
mFOLFOX6 plus cetuximab or panitumumab (only for pan-RAS and BRAF V600E wild-type tumors)
Irinotecan plus cetuximab or panitumumab (only for pan-RAS and BRAF V600E wild-type tumors, and if anti-EGFR therapy was not used in combination with FOLFIRI)
Cetuximab 500 mg/m2 IV over 2 h every 2 weeks or cetuximab 400 mg/m2 IV over 2 h on day 1, then 250 mg/m2 IV over 1 h weekly with reevaluation after 8 wk
Panitumumab 6 mg/kg over 60-90 min every 2 wk with reevaluation after 8 wk
Pembrolizumab 200 mg IV q3wk, in adults with unresectable or metastatic colon cancer that has tested positive for MSI-H or deficient mismatch repair (dMMR) and has progressed following treatment with a fluoropyrimidine (eg, 5-FU, capecitabine), oxaliplatin, and irinotecan
Nivolumab 240 mg IV q2wk, for unresectable or metastatic colon cancer that has tested positive for MSI-H or dMMR and has progressed following treatment with a fluoropyrimidine, oxaliplatin, and irinotecan
Referral for clinical trial
Third-line chemotherapy for metastatic disease:
Panitumumab 6 mg/kg over 60-90 min every 2 wk only for pan-RAS and BRAF V600E wild-type tumors, with reevaluation after 8 wk
Any regimen incorporating an EGFR antibody for patients with pan- RAS wild-type disease, using a cytotoxic backbone not previously tried
Regorafenib 160 mg PO qd for first 21 days of each 28-day cycle
First cycle: Regorafenib 80 mg PO qd on days 1-7, then 120 mg qd on days 8-14, then 160 mg PO qd on days 15-21 of each 28-day cycle; for subsequent cycles give 160 mg qd on days 1-21; monitor hepatic function before and during treatment and interrupt, reduce, or discontinue drug accordingly
Tipiracil/trifluridine 35 mg/m2 PO BID on days 1-5 and days 8-12 of each 28-day cycle; not to exceed 80 mg/dose; for use in patients previously treated with fluoropyrimidine-, oxaliplatin- and irinotecan-based chemotherapy, an anti–vascular endothelial growth factor (VEGF) biological therapy, and (if pan- RAS wild-type), an anti-EGFR therapy
Pembrolizumab 200 mg IV q3wk over 30 min, for adults with unresectable or metastatic colon cancer that has tested positive for MSI-H or dMMR and has progressed following treatment with a fluoropyrimidine (eg, 5-FU, capecitabine), oxaliplatin, and irinotecan
Nivolumab 240 mg IV q2wk over 30 min, for unresectable or metastatic colon cancer that has tested positive for MSI-H or dMMR and has progressed following treatment with a fluoropyrimidine (eg, 5-FU, capecitabine), oxaliplatin, and irinotecan
Nivolumab 3 mg/kg IV over 30 min, followed by ipilimumab 1 mg/kg IV over 30 min on the same day; repeat combination q3Weeks for up to 4 doses, THEN administer nivolumab 250 mg IV q2Weeks until disease progression or unacceptable toxicity.
Referral for clinical trial
Xelox (CAPOX)
For the first- and second-line treatment of advanced colorectal cancer
Capecitabine (Xeloda) 1,000 mg/m2 PO twice daily (approximately 12 hours apart) within 30 minutes after a meal on the evening of day 1 through the morning of day 15 in combination with oxaliplatin (130 mg/m2 IV on day 1), repeated every 3 weeks.
In a phase III trial of 2,034 patients, capecitabine/oxaliplatin (XELOX) with or without bevacizumab was compared with fluorouracil/leucovorin/oxaliplatin (FOLFOX4) with or without bevacizumab in a 2-by-2 factorial design. XELOX was found to be noninferior to FOLFOX4 for the first line treatment of metastatic colorectal cancer (8 months vs. 8.5 months, HR 1.04; 97.5% CI, 0.93 to 1.16).
In the safety analysis of 1,304 patients, grade 3 or 4 adverse reactions observed more frequently with XELOX included diarrhea (grade 3, 19%; grade 4: 1%) and hand-foot syndrome (grade 3, 6%), while FOLFOX4 produced more neutropenia (grade 3, 27%; grade 4, 16%).
A meta-analysis of this trial and 5 additional trials was performed concurrently with this study. No difference in progression-free survival or overall survival was observed between capecitabine/oxaliplatin combinations and fluorouracil/leucovorin/oxaliplatin combinations in patients with metastatic colorectal cancer.
Additional trials have shown efficacy for XELOX in the treatment of both previously treated and previously untreated patients with advanced colorectal cancer.
Capecitabine (Xeloda) + Oxaliplatin Q3W TOI
*Oxaliplatin IV 130 mg/m2 IV infusion over 2 hours Admix fluid: Dextrose 5 % In Water Volume: 250 mL Instructions: Not compatible with NS.
*Capecitabine Oral 1000 mg/m2 BID, (day 1, evening, to day 15, morning). Take with water and within 30 minutes of the end of a meal.
PREMEDICATIONS
Ondansetron IV 16 mg intravenously once.
Dexamethasone IV Dexamethasone 10 mg IV over 20 minutes. Admix fluid: 0.9 % Sodium Chloride Volume: 50 mL.
For the adjuvant treatment of stage III (Dukes C) colon cancer in combination with oxaliplatin (XELOX or CapeOX)†.
Repeated every 3 weeks for a total of 8 cycles.
In a phase III clinical trial, 1,886 patients with resected stage III colon cancer were randomized to receive oxaliplatin/capecitabine (XELOX) or 5-fluorouracil/leucovorin. After a median follow-up of 57 months, the addition of oxaliplatin to capecitabine produced a significant improvement in the primary endpoint, disease-free survival (HR 0.8; p = 0.0045). Disease-free survival at 3 years was 70.9% with XELOX vs. 66.5% with 5-FU/leucovorin. Overall survival was not significantly different between the arms (HR 0.87; p = 0.1486). Grade 3 or 4 neurosensory toxicity, vomiting, hand-foot syndrome, and thrombocytopenia occurred more frequently in the XELOX arm (p < 0.05); neutropenia, febrile neutropenia, and stomatitis occurred more frequently with 5-FU/leucovorin (p < 0.05).]
MOST COMMON SIDE EFFECTS OF CAPOX
Nausea, Vomiting, Diarrhea
Handfoot Syndrome
Neuropathy
For the treatment of unresectable advanced or metastatic biliary tract cancer†.
Multiple dosage regimens have been studied.
Capecitabine 1,250 mg/m2 PO twice daily on days 1 to 14, followed by a 7-day rest period, given in combination with cisplatin 60 mg/m2 IV over 1 hour on day 1, repeated every 21 days until disease progression or unacceptable toxicity.
In a phase II trial of 38 patients, capecitabine/cisplatin produced an overall response rate of 21.4%. Grade III or IV neutropenia occurred in 20% of patients
Another regimen is capecitabine 650 mg/m2 PO twice daily on days 1 to 14, followed by a 7-day rest period, given in combination with gemcitabine 1,000 mg/m2 IV over 30 minutes on days 1 and 8, repeated every 21 days. In phase II trials, this dosage produced an ORR of 29% to 31%.
Another phase II trial of 43 patients studied capecitabine 1,000 mg/m2 PO twice daily on days 1 to 14, followed by a 7-day rest period, given in combination with cisplatin 60 mg/m2 IV on day 1 and epirubicin 50 mg/m2 IV on day 1, repeated every 21 days until disease progression or unacceptable toxicity.
1) For the first-line or second-line treatment of metastatic colorectal cancer
bevacizumab in combination with 5-fluorouracil, leucovorin, and irinotecan (IFL plus bevacizumab).
2) For the first-line treatment of KRAS wild-type, EGFR-expressing, metastatic colorectal cancer (mCRC)
cetuximab in combination with FOLFIRI (irinotecan, 5-fluorouracil, leucovorin).
NOTE: In clinical trials, response rates did not correlate with either the percentage of EGFR positive cells or the intensity of EGFR expression. EGFR expression status and the absence of a Ras mutation should be determined by an FDA approved test prior to starting therapy
(http://www.fda.gov/medicaldevices/productsandmedicalprocedures/invitrodiagnostics/ucm301431.htm)
NCCN preferred: bevacizumab + irinotecan
Cancer Chemother Pharmacol. 2017 Mar;79(3):579-585. doi: 10.1007/s00280-017-3255-3. Epub 2017 Feb 17.
https://www.ncbi.nlm.nih.gov/pubmed/28213683
Phase II study of bevacizumab and irinotecan as second-line therapy for patients with metastatic colorectal cancer previously treated with fluoropyrimidines, oxaliplatin, and bevacizumab.
Abstract
PURPOSE:
Fluorouracil and folinic acid with irinotecan (FOLFIRI) plus bevacizumab (BV) is widely used as second-line chemotherapy for patients with metastatic colorectal cancer (mCRC) previously treated with fluoropyrimidines, oxaliplatin, and BV. FOLFIRI requires a CV catheter and an infusion pump, which are inconvenient for patients. Sufficient data are not available for characterizing the effectiveness of fluoropyrimidines beyond first disease progression. In this study, we evaluated the efficacy and safety of irinotecan (CPT-11) plus BV as second-line therapy.
METHODS:
Patients with mCRC previously treated with at least four courses of a fluoropyrimidine, oxaliplatin, and BV were designated to receive 150 mg/m2 of CPT-11 and 10 mg/kg of BV every 2 weeks as second-line therapy. The primary endpoint was progression-free survival (PFS), and secondary endpoints included response rate (RR), overall survival (OS), and adverse events.
RESULTS:
Thirty patients from six institutes were enrolled from March 2011 to January 2014. The median PFS was 5.7 months (95% CI 4.2-7.3 months), and the RR was 6.7% (range 0.8-22.1%). Grades 3-4 adverse events included leucopenia (36.7%), neutropenia (50%), thrombocytopenia (26.7%), anemia (30%), diarrhea (3.3%), anorexia (6.7%), and hypertension (3.3%). Relative dose intensities were 94.5 and 96.3% for CPT-11 and BV, respectively. The median OS was 11.8 months (6.3 months-not reached).
CONCLUSIONS:
Administration of CPT-11 plus BV to patients with mCRC achieved comparable efficacies with relatively lower toxicities compared with the results of previous studies using FOLFIRI plus BV as second-line therapy. The dose intensity of CPT-11 was judged as satisfactory.
Summary - Drug therapy of Advanced Colon Cancer
First Line RAS/BRAF/MSI testing, Sidedness
Chemotherapy: 1. fluoropyrimidine/oxaliplatin regimen
2. Irinotecan regimen
Anti-Angiogenesis
◦ bevacizumab (Avastin) + Chemotherapy
Epidermal growth factor receptor (EGFR) inhibitors
◦ cetuximab (Erbitux) + Chemotherapy
◦ panitumumab (Vectibix) + Chemotherapy
Tumor with non-mutated, KRAS wild-type.
Second or Third Line
Anti-Angiogenesis
◦ ramucirumab (Cyramza) + Chemotherapy
◦ regorafenib (Stivarga) + Chemotherapy
◦ ziv-aflibercept (Zaltrap) + Chemotherapy
ziv-aflibercept (Zaltrap) was given with FORFIRI
for patients previously treated with oxaliplatin.
BRAF positive, RAS WT
vemurafenib + Irinotecan + cetuximab
Second or Third Linee MSI/PDL1 testing
MSI-H/dMMR :
◦ pembrolizumab (Keytruda)
◦ nivolumab (Opdivo)
PDL1 positive:
◦ pembrolizumab (Keytruda)
◦ nivolumab (Opdivo)
Further somatic profiling.
Refractory Colon Cancer
◦ TAS 102
◦ regorafenib (Stivarga)
◦ HER2 as a target
TAS-102, a combination of triflurothymidine
and the thymidine phosphorylase inhibitor TPI,
is active in 5FU-resistant tumors.
Molecular Markers in Colon Cancer
Microsatellite Instability
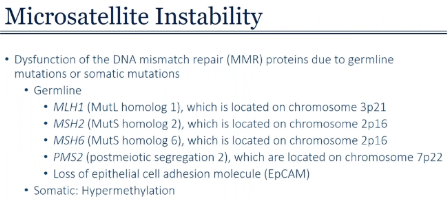
MSI & Tumor-associated inflammatory response
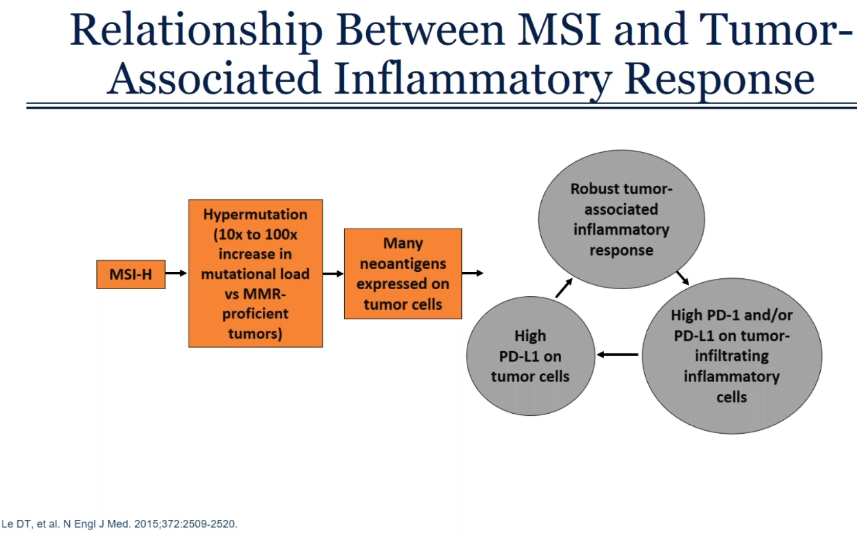
EGFR Biomarker Evolution
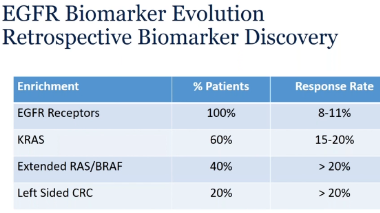
Side Effects of Chemothrapy
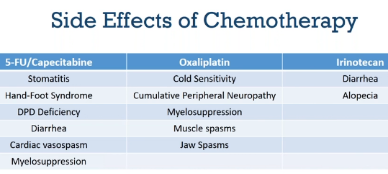
Side Effects of Targeted Therapy/Immunotherapy
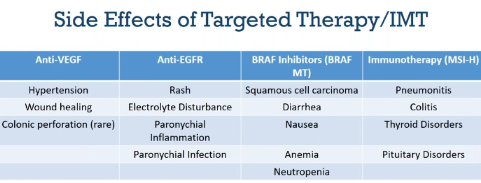
Dermatologic toxicity in EGFR Targeted Therapy
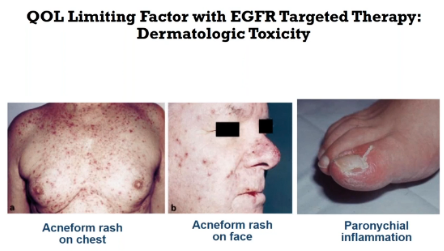
Colorectal Cancer Practice Changes 2017
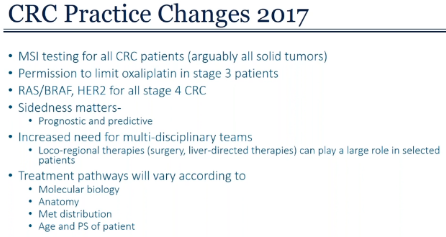
Surgery cures some patients with stage IV Colorectal cancer.
RFA can ablate liver metastatic lesions.
RT and Embo less reliably ablate liver metastatic lesions.
Peri-operative chemo can only cure few patients.
Only fluoropyrimidine and oxaliplatin have curative potential in the adjuvant setting.
NCCN Guidelines for Colon Cancer
Colorectal cancer (CRC) is the fourth most frequently diagnosed cancer and the second leading cause of cancer death in the United States.
The incidence and mortality of CRC has been declining.
These improvements in incidence of and mortality from CRC are thought to be a result of shifting patterns of CRC risk factors, cancer prevention and earlier diagnosis through screening, and better treatment modalities.
Despite the observed improvements in the overall CRC incidence rate, its incidence in patients aged <50 years has been increasing. The cause of this trend is currently unknown.
Adjuvant Treatment
Adjuvant therapy may confer a survival advantage in some patients with resected colon cancer (eg, those with stage III or high-risk stage II disease).
However, adjuvant treatment, especially with regimens containing oxaliplatin, is associated with considerable toxicity (notably chemotherapy-induced peripheral neuropathy), and not all patients derive benefit.
Consideration of disease stage and pathologic features, microsatellite instability (MSI) status, possible efficacy and toxicity profiles associated with treatment choice, and patient age, comorbidities, and preferences aid in decision-making regarding the use of adjuvant therapy for patients with colon cancer.
The IDEA collaboration investigated whether a shortened duration of adjuvant therapy would be a feasible way to avoid or lessen toxicities associated with oxaliplatin-containing adjuvant therapy in some patients with locoregional colon cancer, without impairing oncologic outcomes.
The data were sufficient to warrant division of stage III colon cancer into a low-risk (T1–3, N1) and a high-risk group (T4, N1–2 or Any T, N2)
For the low-risk group, the recommended duration of adjuvant therapy is 3 months if CapeOX is chosen, because noninferiority for DFS was proven in IDEA and patients should be spared the increased toxicity, cost, and inconvenience of longer therapy.
If FOLFOX is chosen for these patients, then 3 to 6 months of FOLFOX is recommended. The panel believes the shorter duration can be considered to reduce toxicity, cost, and inconvenience, but noninferiority could not be proven for 3 versus 6 months of FOLFOX in this subset.
For patients with high-risk stage III colon cancer, 3 to 6 months of adjuvant therapy is recommended if CapeOX is chosen; noninferiority of the shorter duration was not proven in this subset of patients, but the panel believes the shorter duration can be considered to minimize toxicity, cost, and inconvenience. Furthermore, DFS with 3 months of therapy was noninferior to DFS with 6 months for the entire cohort (Tany, N1–2) who received CapeOX (HR, 0.95; 95% CI, 0.85–1.06).
Finally, FOLFOX, if chosen, should be given for a full 6 months in the high-risk group because 3 months was shown to be inferior to 6 months for DFS.
The panel then discussed some concerns about the dosing of capecitabine in CapeOX, which they believe is critical if the decision is to give 3 months of CapeOX. Many oncologists, especially in the United States, routinely reduce the starting dose of capecitabine, but the panel strongly believes that the starting dose used in IDEA8 (1,000 mg/m2 twice daily) should be used because it is the only validated dose. The panel also discussed that, in practice, oxaliplatin is dropped from FOLFOX and CapeOX after 6 to 10 doses to reduce the risk of severe neurotoxicity. Therefore, it may be reasonable to complete 3 months of CapeOX for patients with high-risk stage III colon cancer and then drop oxaliplatin and continue capecitabine. However, the panel was divided on whether to recommend this approach.
The NCCN Guidelines list FOLFOX and CapeOX as equally preferred options without strongly recommending one over the other. Efficacy is similar, FOLFOX is less expensive for US patients, and CapeOX is more convenient for most patients (especially 3 months of CapeOX vs 6 months of FOLFOX). Both regimens are preferred over the other options for adjuvant treatment of patients with stage III colon cancer—6 months of either capecitabine or 5-FU/leucovorin—which are generally only recommended for patients with stage III colon cancer if they cannot tolerate oxaliplatin.
| Pathologic Stage | Adjuvant Treatment | |
| TIS, T1, T2, T3 | N0, M0 | Observation |
| T3 MSL-L or MSS No high-risk features |
N0, M0 | Observation OR 5 FU/LV or Capecitabine |
| T3 (High-risk) OR T4 |
N0, M0 | Observation OR 5 FU/LV or Capecitabine OR CAPEOX or FOLFOX |
| T1, T2, T3 (Low-risk stage III) |
N1, M0 | CAPEOX (3 months)** or FOLFOX (3-6 months)**(Category 1 for 6 months) OR Other options: 5FU (6 months) or Capecitabine (6 months) |
| T4 (High-risk stage III) |
N1-2, M0 | CAPEOX (3-6 months)**(Category 1 for 6 months) or FOLFOX (6 months)**(Category 1) (Consider RT for T4 with penetration to a fixed structure) OR Other options: 5FU (6 months) or Capecitabine (6 months) (Consider RT for T4 with penetration to a fixed structure) |
| Any T (High-risk stage III) |
N2, M0 | |
** Addition of Oxaliplatin has not been proved to be benefit in pts age 70 & older.
Despite the large number of patients in IDEA, the results were not as definitive as the panel would require for these new recommendations to be listed as category 1. Therefore, these shorter durations are included in the guidelines as category 2A recommendations. The 6-month durations of FOLFOX or CapeOX for patients with stage III colon cancer remain as category 1 recommendations based on older trials.
Note: Oxaliplatin is associated with cumulative dose‐dependent neurotoxicity
• Debilitating for many patients, both short‐ and long‐term
Nerve damage (e.g. numbness, tingling, pain) can persist long after discontinuation of therapy, sometimes permanently
Dose reductions and early discontinuation of therapy are common
• Shorter duration of treatment without loss of efficacy would be of benefit to patients and health care resources
Treatment of RAS Wild-Type/BRAF Mutation–Positive Metastatic CRC
Although survival for patients with advanced CRC has improved dramatically over the past decades, the most recently reported 5-year survival rate for patients with stage IV CRC was only 14%. Moreover, patients with BRAF-mutated mCRC have a particularly poor prognosis. BRAF V600E mutations are present in approximately 8% of mCRC cases and are associated with a more aggressive biology, shorter OS, and decreased response to chemotherapy compared with BRAF wild-type tumors. Thus, additional treatment options are still needed in mCRC, especially for the BRAF mutation–positive subset of patients.
Vemurafenib selectively inhibits the V600E-mutated form of the BRAF kinase.
However, vemurafenib monotherapy has shown limited activity in mCRC. Preclinical data suggest that BRAF V600E inhibition alone is ineffective because feedback activation of EGFR occurs. Therefore, blockage of EGFR and BRAF V600E together has been speculated to be more effective than BRAF V600E inhibition alone.
However, vemurafenib in combination with cetuximab- or panitumumab-based therapy has been ineffective in early clinical trials. Results from preclinical and early clinical studies suggest that the addition of irinotecan to BRAF and EGFR inhibition may improve antitumor activity.
The combination of vemurafenib, cetuximab, and irinotecan was thus tested in patients with BRAF V600E–mutated mCRC in the phase II SWOG S1406 trial.
The panel felt that the data from SWOG S1406 were strong enough to warrant the addition of vemurafenib/cetuximab/irinotecan for patients with BRAF V600E–mutated mCRC at this time.
In general, the panel believes that panitumumab and cetuximab are interchangeable.
They do not believe that dabrafenib and vemurafenib are interchangeable.
The panel declined to add dabrafenib/(cetuximab or panitumumab)/irinotecan to the continuum of care for patients with BRAF-mutant mCRC.
With the addition of vemurafenib/(cetuximab or panitumumab)/irinotecan to the mCRC continuum of care, the BRAF status of the tumor is now another factor that must be considered when choosing therapies for patients with mCRC.
The panel further notes that BRAF and RAS mutations are mutually exclusive. Therefore, although the guidelines only indicate that the new regimens are for “BRAF V600E mutation–positive” disease, these patients' tumors contain wild-type RAS.
In mCRC, data from the SWOG S1406 trial has led to new treatment options specifically for patients with BRAF V600E–mutated tumors. These patients have derived little benefit from EGFR-targeted agents in the past and have had poor prognoses. The addition of an inhibitor of the specific BRAF mutation provides additional treatment options that include EGFR inhibitors and gives these patients a chance for delayed disease progression.
Principles of Pathologic Review and Biomarker Testing
www.jnccn.org Principles of Pathologic Review and Biomarker Testing Copy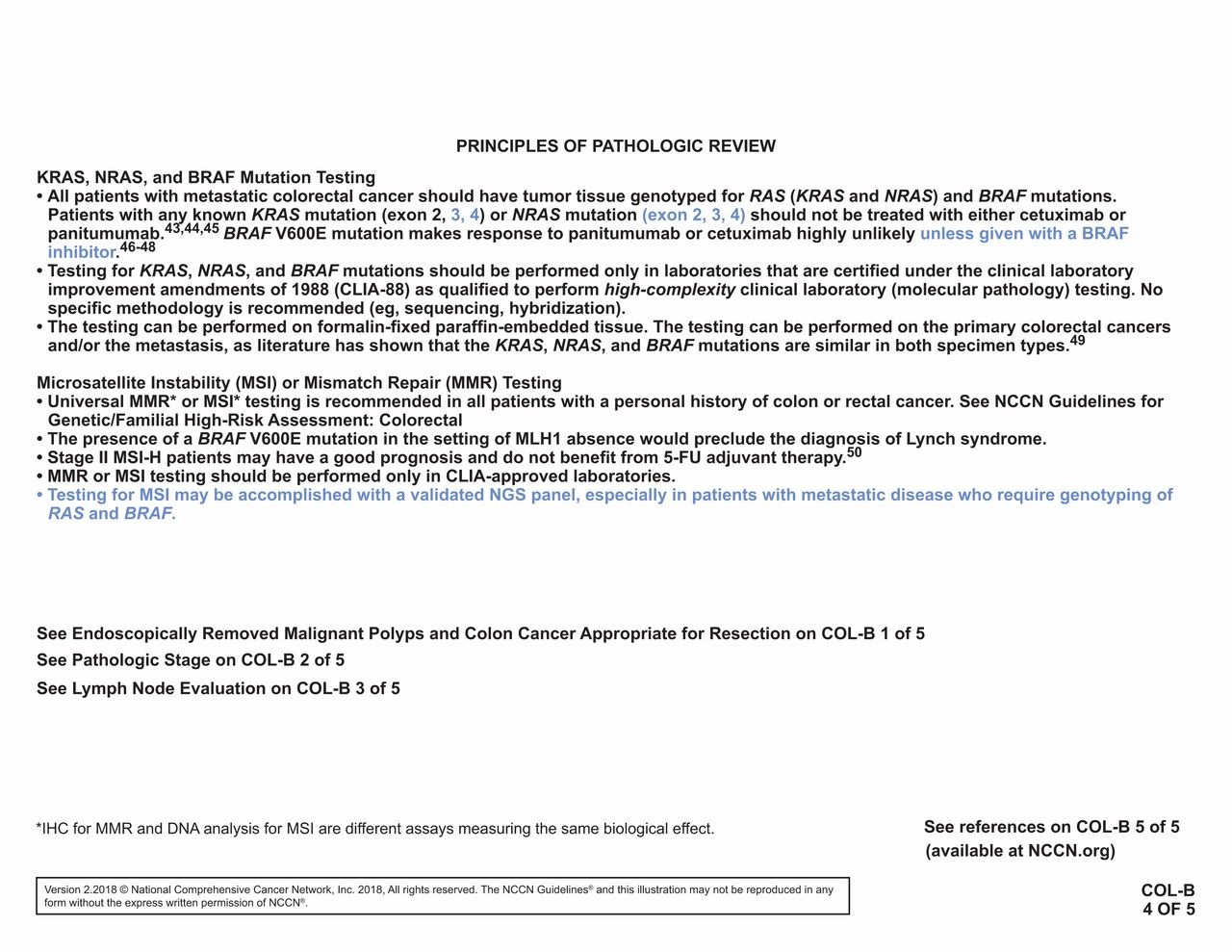{kind=link}
Treatment Options for unresectable metachronous metastasis
I.
• No previous chemotherapy
• Previous 5 FU/LV or Capecitabine
• Previous adjuvant CAPEOX/FOLFOX >12 months
Recommendation:
Systemic chemotherapy with CAPEOX/FOLFOX
Re-evaluate for resectability every 2 months.
• Previous adjuvant CAPEOX/FOLFOX within 12 months
Recommendation:
• FOLFIRI/Irinotecan ± anti-angiogenetic agents (bevacizumab**, ramucirumab, or ziv-aflibercept); OR
• FOLFIRI/Irinotecan ± anti-EGFR (cetuximab or panitumumab)- WT KRAS/NRAS*** only; OR
• Irinotecan + cetuximab/panitumumab + vemurafenib (BRAF V600E mutation positive***); OR
• nivolumab or pembrolizumab (dMMR/MSI-H only)
Re-evaluate for resectability every 2 months.
II.
Patients are re-evaluated every 2 months.
If the tumor remains unresectable, then continue the drug therapy.
If the tumor converts to resectability, then surgery can be done and followed by observation or adjuvant therapy (Chemotherapy ± Biologic therapy).
Hepatic artery infusion ± 5FU/LV (Categoer 2B) is also an option.
** bevacizumab is the preferred anti-angiogenic agents based on toxicity &/or cost.
*** BRAF V600E mutation makes response to cetuximab or panitumumab highly unlikely.
Systemic Therapy for Advanced or Metastatic Colon Cancer
1st line: Oxaliplatin-based therapy if not previously given - e.g., FOLFOX, CapeOX
2nd line: Irinotecan-based therapy
• FOLFIRI or Irinotecan; OR
• FOLFIRI/Irinotecan + anti-angiogenetic agents (bevacizumab**, ramucirumab, or ziv-aflibercept); OR
• FOLFIRI/Irinotecan + anti-EGFR (cetuximab or panitumumab)- WT KRAS/NRAS*** only; OR
• Irinotecan + cetuximab/panitumumab + vemurafenib (BRAF V600E mutation positive***); OR
• nivolumab or pembrolizumab (dMMR/MSI-H only)
3rd line:
• regorafenib; OR
• Trifluridin + tipiracil; OR
• nivolumab or pembrolizumab (dMMR/MSI-H only) OR
• Best supportive Care
SYSTEMIC THERAPY FOR ADVANCED OR METASTATIC DISEASE
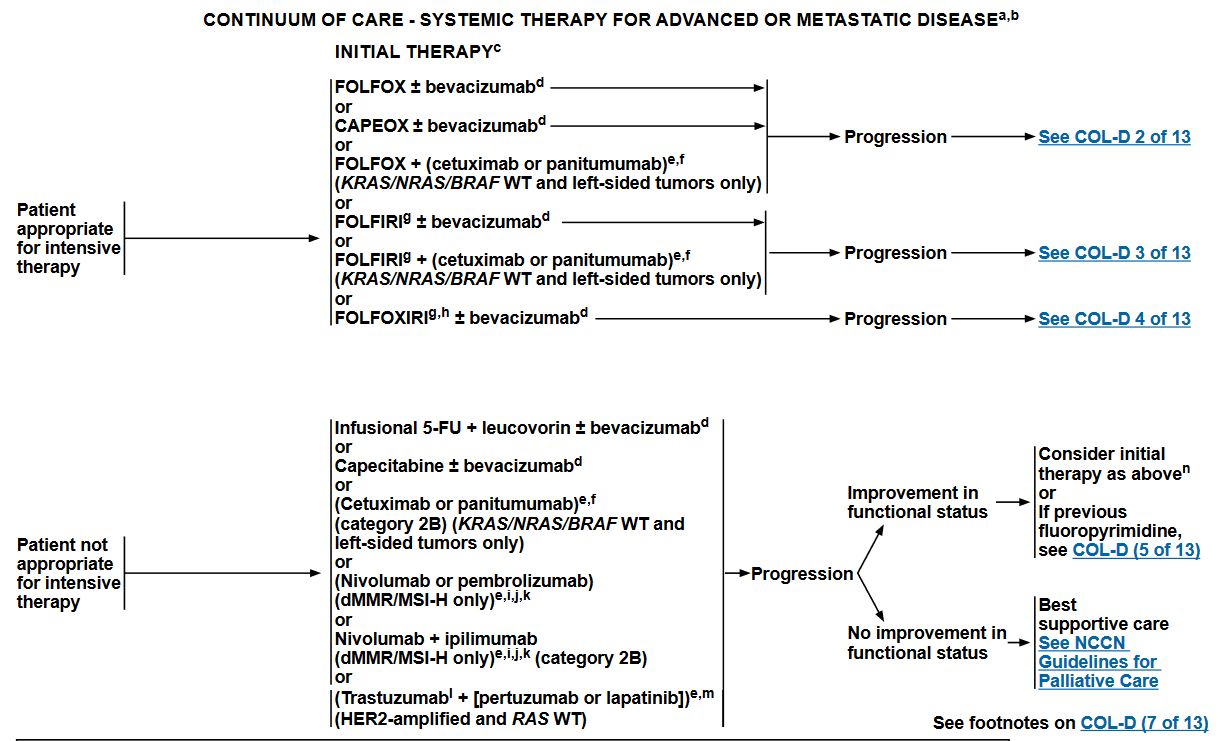
SYSTEMIC THERAPY FOR ADVANCED OR METASTATIC DISEASE
Patient appropriate for intensive therapy
Oxaliplatin-based therapy --> Progression -->COL-D2
CAPEOX ± bevacizuma
FOLFOX ± bevacizumab
FOLFOX + (cetuximab or panitumumab) = (KRAS/NRAS/BRAF WT and left-sided tumors only)
Irinotecan-based therapy --> Progression -->COL-D3
FOLFIRI ± bevacizumab -->COL-D3
FOLFIRI + (cetuximab or panitumumab) = (KRAS/NRAS/BRAF WT and left-sided tumors only)
Oxaliplatin and Irinotecan-based therapy --> Progression -->COL-D4
FOLFOXIRI ± bevacizumab
Patient not appropriate for intensive therapy
Infusional 5-FU + leucovorin ± bevacizumabd
Capecitabine ± bevacizumab
(Cetuximab or panitumumab) (category 2B) = (KRAS/NRAS/BRAF WT and left-sided tumors only)
(Nivolumab or pembrolizumab) = (dMMR/MSI-H only)
Nivolumab + ipilimumab = (dMMR/MSI-H only) (category 2B)
(Trastuzumabl + [pertuzumab or lapatinib]) = (HER2-amplified and RAS WT)
Previous oxaliplatin-based therapy
FOLFIRI or irinotecan
+ (bevacizumabd, [preferred] or
+ ziv-aflibercept or
+ ramucirumab
OR
(FOLFIRI or irinotecan) + (cetuximab or panitumumab) = (KRAS/NRAS/BRAF WT only)
(Dabrafenib + trametinib) + (cetuximab or panitumumab) = (BRAF V600E mutation positive)
Encorafenib + (cetuximab or panitumumab) ± binimetinib = (BRAF V600E mutation positive)
OR
[Nivolumab ± ipilimumab] or pembrolizumab = (dMMR/MSI-H only)
(Trastuzumabl + [pertuzumab or lapatinib]) = (HER2-amplified and RAS WT)
Third-line include:
Regorafenib
Trifluridine + tipiracil
Previous irinotecan-based therapy
FOLFOX or CAPEOX
FOLFOX + bevacizumabd
CAPEOX + bevacizumab
FOLFOX + (cetuximab or panitumumab) = (KRAS/NRAS/BRAF WT only)
OR
Irinotecan + (cetuximab orpanitumumab) = (KRAS/NRAS/BRAF WT only)
(Dabrafenib + trametinib) + (cetuximab or panitumumab) = (BRAF V600E mutation positive)
Encorafenib + (cetuximab or panitumumab) ± binimetinib = (BRAF V600E mutation positive)
OR
[Nivolumab ± ipilimumab] or Pembrolizumab = dMMR/MSI-H only
Trastuzumabl + [pertuzumab or lapatinib] = (HER2-amplified and RAS WT)
Third-line include:
Regorafenib
Trifluridine + tipiracil